You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Atlas de Anatomie A Omului McMinnDocument340 pagesAtlas de Anatomie A Omului McMinnoana_4u_89702495% (110)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Sinelnikov - Atlas of Human Anatomy - Volume 2 - Part 2Document217 pagesSinelnikov - Atlas of Human Anatomy - Volume 2 - Part 2İsmail Şimşek0% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Sinelnikov - Atlas of Human Anatomy - Volume 2 - Part 2Document217 pagesSinelnikov - Atlas of Human Anatomy - Volume 2 - Part 2İsmail Şimşek0% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Sinelnikov Vol 1Document437 pagesSinelnikov Vol 1Freezy Frizzle94% (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Ch27 Urinary SystemDocument52 pagesCh27 Urinary Systemİsmail ŞimşekNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Human Anatomy,: First Edition Mckinley & O'LoughlinDocument65 pagesHuman Anatomy,: First Edition Mckinley & O'Loughlinİsmail ŞimşekNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 25Document41 pages25dewkmcNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 33 Heme MetabolismDocument1 page33 Heme Metabolismİsmail ŞimşekNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- BIOL226Lec09 - Abdominal VesselsDocument99 pagesBIOL226Lec09 - Abdominal Vesselsİsmail ŞimşekNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Essentials of Human Anatomy and Physiology: Chapter 10: The Endocrine SystemDocument35 pagesEssentials of Human Anatomy and Physiology: Chapter 10: The Endocrine Systemİsmail ŞimşekNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Essentials of Anatomy and Physiology: Chapter 7: Muscular SystemDocument9 pagesEssentials of Anatomy and Physiology: Chapter 7: Muscular Systemİsmail ŞimşekNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 38 Metabolic Pathways 2Document1 page38 Metabolic Pathways 2İsmail ŞimşekNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Biochimie MetabolismDocument2 pagesBiochimie MetabolismSaca AnastasiaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- 28 Folic Acid C1 PoolDocument1 page28 Folic Acid C1 Poolİsmail ŞimşekNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
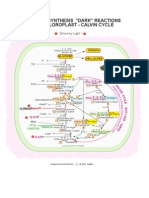
- 27 Calvin CycleDocument1 page27 Calvin Cycleİsmail ŞimşekNo ratings yet
- 22 Pentose Phosohate Pathways 2Document1 page22 Pentose Phosohate Pathways 2İsmail ŞimşekNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Second Division People of The PhilippinesDocument187 pagesSecond Division People of The PhilippinesLuigi JaroNo ratings yet
- Design and Development of A Hand Exoskeleton For Rehabilitation of Hand Injuries 2014Document14 pagesDesign and Development of A Hand Exoskeleton For Rehabilitation of Hand Injuries 2014newkid2202No ratings yet
- Bony ThoraxDocument6 pagesBony ThoraxKaren LaureanoNo ratings yet
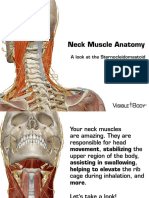
- Neck Muscles 041715 PDFDocument15 pagesNeck Muscles 041715 PDFJohn DavidNo ratings yet
- G.B.-36 Outer Mound WAIQIU - Acupuncture Points: Admin Comments 0Document11 pagesG.B.-36 Outer Mound WAIQIU - Acupuncture Points: Admin Comments 0224118No ratings yet
- Shoulder MobilizationsDocument33 pagesShoulder MobilizationsEASHWARNo ratings yet
- Visible Body 3D Human Anatomy Atlas Controls - ManualDocument5 pagesVisible Body 3D Human Anatomy Atlas Controls - ManualMiruna A. CopoiuNo ratings yet
- Ns Elec 4 - Musculo-Skeletal SystemDocument7 pagesNs Elec 4 - Musculo-Skeletal SystemONGLENGCO WILSON JAKE V.No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Natural Desing PDFDocument7 pagesNatural Desing PDFIlseNo ratings yet
- Dwnload Full Nursing Assistant A Nursing Process Approach 11th Edition Acello Solutions Manual PDFDocument35 pagesDwnload Full Nursing Assistant A Nursing Process Approach 11th Edition Acello Solutions Manual PDFmichaelcalhounjtypaegbnk100% (11)
- Diplo Verte BronDocument4 pagesDiplo Verte BronAsepZeryKusmayaNo ratings yet
- Pampas Cat GroupDocument36 pagesPampas Cat GrouppristidactylusNo ratings yet
- Tibio-Tarsal Luxation and Its Management in A Dog: Ayyappan, S., M. Shiju Simon, B. C. Das and R. Suresh KumarDocument4 pagesTibio-Tarsal Luxation and Its Management in A Dog: Ayyappan, S., M. Shiju Simon, B. C. Das and R. Suresh KumarEnnur NufianNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Revision of The South American Wasp Genus Aelurus (Hymenoptera: Tiphiidae: Thynninae)Document15 pagesRevision of The South American Wasp Genus Aelurus (Hymenoptera: Tiphiidae: Thynninae)Francisco Rojas EspinozaNo ratings yet
- Lingual ArchDocument2 pagesLingual ArchDr.Prakher SainiNo ratings yet
- Core Curriculum Sonographic Scanning PlanesDocument37 pagesCore Curriculum Sonographic Scanning PlanesPop Nice100% (1)
- Lecture 4 - A&P - Basic Anatomical TerminologyDocument30 pagesLecture 4 - A&P - Basic Anatomical TerminologyNur ShamrinzNo ratings yet
- Anatomy and PhysiologyDocument49 pagesAnatomy and PhysiologyAnthonio Muenho100% (1)
- Symmetry of Skin TemperatureDocument4 pagesSymmetry of Skin TemperaturepenfoNo ratings yet
- Intraosseous Infusion - UpToDateDocument31 pagesIntraosseous Infusion - UpToDatehatsuneNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- AnthropometryDocument172 pagesAnthropometryAntonio C. Keith100% (1)
- Barouk Countersink Screw From Biomet PDFDocument36 pagesBarouk Countersink Screw From Biomet PDFJacob DoughertyNo ratings yet
- Introduction To Bio Mechanics Slide ShowDocument35 pagesIntroduction To Bio Mechanics Slide ShowOnwaree Ing100% (2)
- FR Radius UlnaDocument49 pagesFR Radius UlnaEkha SaraswatiNo ratings yet
- Fascial SpacesDocument79 pagesFascial SpacesArun MamachanNo ratings yet
- Test Bank For High Acuity Nursing 7th Edition WagnerDocument36 pagesTest Bank For High Acuity Nursing 7th Edition Wagnermurlinsquadrantygbh0v100% (45)
- Fish IdentificationDocument18 pagesFish IdentificationMujahid Hussain100% (1)
- Case DigestDocument100 pagesCase DigestAys100% (1)
- Anatomical Terms and Planes PDFDocument3 pagesAnatomical Terms and Planes PDFAshera Queenielet MagbooNo ratings yet
- RENAL Nephrometry Scoring System: The Radiologist's PerspectiveDocument5 pagesRENAL Nephrometry Scoring System: The Radiologist's PerspectiveGaltieri OtavioNo ratings yet