You might also like
- Alkaptonuria: Rare Genetic Disorder Causing Dark Urine and Joint ProblemsDocument32 pagesAlkaptonuria: Rare Genetic Disorder Causing Dark Urine and Joint ProblemsKrishnamurthy VenkatachalamNo ratings yet
- AlkaptonuriaDocument5 pagesAlkaptonuriaDiana SanchezNo ratings yet
- AlkaptonuriaDocument12 pagesAlkaptonuriaGirish Kishor PaiNo ratings yet
- New Developments in Ochronosis: Review of The LiteratureDocument6 pagesNew Developments in Ochronosis: Review of The LiteratureHadi FirmansyahNo ratings yet
- Physiological Aspects of AgeingDocument5 pagesPhysiological Aspects of AgeingFelipe RojasNo ratings yet
- Alport SyndromeDocument7 pagesAlport SyndromeNTA UGC-NET100% (1)
- What is Alkaptonuria? Rare Genetic Disorder Causes Dark Urine & Joint ProblemsDocument4 pagesWhat is Alkaptonuria? Rare Genetic Disorder Causes Dark Urine & Joint ProblemsJustin PerezNo ratings yet
- Spirovital Therapy Option For Macular DegenerationDocument6 pagesSpirovital Therapy Option For Macular DegenerationtavlarNo ratings yet
- Gene Mutations Caused by Radiation: PKU, Hemochromatosis, TelangiectasiaDocument12 pagesGene Mutations Caused by Radiation: PKU, Hemochromatosis, TelangiectasiaTyrone Stavros BarracaNo ratings yet
- ALKAPTONURIADocument15 pagesALKAPTONURIAJean Claude Balancio100% (1)
- Reviews in Clinical GerontologyDocument18 pagesReviews in Clinical GerontologyRADYA PUTRA PRATAMANo ratings yet
- Developmental Defects Causes and TypesDocument10 pagesDevelopmental Defects Causes and TypesChristiNo ratings yet
- Cataract, Senile: Author: Vicente Victor D Ocampo JR, MD, Head, Uveitis and Ocular ImmunologyDocument7 pagesCataract, Senile: Author: Vicente Victor D Ocampo JR, MD, Head, Uveitis and Ocular ImmunologyDicki Pratama HolmesNo ratings yet
- Alport'S SyndromeDocument8 pagesAlport'S SyndromeHemanth PrakashNo ratings yet
- OtosclerosisDocument36 pagesOtosclerosisShamsheer ShaikNo ratings yet
- Moon Face Buffalo Hump Truncal ObesityDocument6 pagesMoon Face Buffalo Hump Truncal ObesityalvincabatoNo ratings yet
- OtosclerosisDocument9 pagesOtosclerosisHelgaNo ratings yet
- O To SclerosisDocument9 pagesO To SclerosisHelgaNo ratings yet
- Top 10 Environmental and Nutrition Disorders PDFDocument87 pagesTop 10 Environmental and Nutrition Disorders PDFAdrian CaballesNo ratings yet
- Achalasia and AchondroplasiaDocument3 pagesAchalasia and AchondroplasiaMarco Antonio WellisNo ratings yet
- Pediatric Organophosphates Toxicity GuideDocument1 pagePediatric Organophosphates Toxicity GuideJC HernándezNo ratings yet
- Asfiksia-Forensik English ClassDocument34 pagesAsfiksia-Forensik English ClassfixyNo ratings yet
- Negative Physiological Changes of AgingDocument27 pagesNegative Physiological Changes of AgingShaharyar100% (1)
- Case Discussion - GlaucomaDocument5 pagesCase Discussion - GlaucomatwelvefeetNo ratings yet
- Secondary GlaucomaDocument19 pagesSecondary GlaucomaRakhmad TriharsadiNo ratings yet
- Revision Topics in OtologyDocument294 pagesRevision Topics in OtologyDr. T. Balasubramanian100% (3)
- Otosclerosis ExplainedDocument12 pagesOtosclerosis ExplainedAhmed MorsyNo ratings yet
- Homeo Eye DiseaseDocument15 pagesHomeo Eye DiseaseAlbena Trifonova100% (3)
- Exophthalmos Is Defined in DorlandDocument15 pagesExophthalmos Is Defined in DorlandAmin Kamaril Wahyudi ArrdianNo ratings yet
- Central Pontine Myelinolysis and The Osmotic Demyelination 2021Document10 pagesCentral Pontine Myelinolysis and The Osmotic Demyelination 2021Nicolas RodriguezNo ratings yet
- Pathophysiology GuidelineDocument82 pagesPathophysiology GuidelineKayla Edwards100% (3)
- Study of The Disease AchondraplasiaDocument5 pagesStudy of The Disease AchondraplasiaEries Lacanlale LumbaNo ratings yet
- Oxidative Damage and The Prevention ofDocument11 pagesOxidative Damage and The Prevention ofFernando NugrohoNo ratings yet
- NBME 11 Answers To All Sections 2Document97 pagesNBME 11 Answers To All Sections 2hussainalmusawiNo ratings yet
- Exophthalmos (Proptosis) - Background, Pathophysiology, EpidemiologyDocument7 pagesExophthalmos (Proptosis) - Background, Pathophysiology, EpidemiologyAbdullah QayyumNo ratings yet
- Goodman & Snyder: Differential Diagnosis For Physical Therapists, 5th EditionDocument2 pagesGoodman & Snyder: Differential Diagnosis For Physical Therapists, 5th EditionZainab WaqarNo ratings yet
- ThanatologyDocument68 pagesThanatologyniraj_sd100% (1)
- Effect of selenium, mercury, and propranolol on chick embryo developmentDocument1 pageEffect of selenium, mercury, and propranolol on chick embryo developmentmolla e embelNo ratings yet
- 1pdb2d1Document12 pages1pdb2d1anitaabreu123No ratings yet
- Histology Stain GuideDocument9 pagesHistology Stain GuideSheba Dan de WiseNo ratings yet
- Theories of AgingDocument55 pagesTheories of AgingUlaim UsmanNo ratings yet
- MedulloblastomaDocument2 pagesMedulloblastomaMohammadAwitNo ratings yet
- Practical exam autopsy questionsDocument31 pagesPractical exam autopsy questionselavelenosaNo ratings yet
- Course: Course Title: Course Credits: Contact Hours/week: Course DescriptionDocument24 pagesCourse: Course Title: Course Credits: Contact Hours/week: Course DescriptionNathaniel PulidoNo ratings yet
- Assessment of The Frail Elderly Client: A. Skin, Hair, and NailsDocument11 pagesAssessment of The Frail Elderly Client: A. Skin, Hair, and Nailsshannon c. lewisNo ratings yet
- Biological and Cognitive Aspects of AgingDocument16 pagesBiological and Cognitive Aspects of AgingAmanda ScarletNo ratings yet
- AP Bio Nucleus Replacement CampaignDocument6 pagesAP Bio Nucleus Replacement CampaignRosa AdamesNo ratings yet
- Achondroplasia: September 2012Document7 pagesAchondroplasia: September 2012ancillaagrayn100% (1)
- Introduction To Radiologic PathologyDocument41 pagesIntroduction To Radiologic PathologyPaul OrtegaNo ratings yet
- Nbme 11Document102 pagesNbme 11Mohamed Nabil100% (36)
- Otosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandOtosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Sarcoidosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandSarcoidosis, A Simple Guide To The Condition, Treatment And Related DiseasesRating: 5 out of 5 stars5/5 (1)
- Preclinical Pathology Review 2023: For USMLE Step 1 and COMLEX-USA Level 1From EverandPreclinical Pathology Review 2023: For USMLE Step 1 and COMLEX-USA Level 1Rating: 5 out of 5 stars5/5 (1)
- Cyanosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCyanosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Necropsy Guide for Dogs, Cats, and Small MammalsFrom EverandNecropsy Guide for Dogs, Cats, and Small MammalsSean P. McDonoughRating: 4 out of 5 stars4/5 (1)
- The Slim Book of Health Pearls: Symptoms Never to IgnoreFrom EverandThe Slim Book of Health Pearls: Symptoms Never to IgnoreNo ratings yet
- Diversity in IndiaDocument24 pagesDiversity in Indiaajithlal_k_k1758No ratings yet
- Train Timing at KozhikodeDocument1 pageTrain Timing at Kozhikodeajithlal_k_k1758No ratings yet
- Enat O9 - : Physics - Part IDocument20 pagesEnat O9 - : Physics - Part Iajithlal_k_k1758No ratings yet
- Mark MbbsDocument48 pagesMark Mbbsajithlal_k_k1758100% (3)
- Learning Strand I - EnglishDocument19 pagesLearning Strand I - EnglishMaricel MaapoyNo ratings yet
- 7 HO Clearance Consent FormDocument2 pages7 HO Clearance Consent FormzanehfncbusinessNo ratings yet
- Bio Brain Review Q S PDFDocument22 pagesBio Brain Review Q S PDFtehilashiftehNo ratings yet
- Bams 1st Rachna Sharir Joints and Their Classification 16-05-2020Document15 pagesBams 1st Rachna Sharir Joints and Their Classification 16-05-2020Sanjana SajjanarNo ratings yet
- IEPF Authority (Recruitment, Salary and Other Terms and Conditions of Service Officers and Other Employees), Rules 2016Document10 pagesIEPF Authority (Recruitment, Salary and Other Terms and Conditions of Service Officers and Other Employees), Rules 2016Latest Laws TeamNo ratings yet
- Nadilla Choerunnisa 2B S.KepDocument3 pagesNadilla Choerunnisa 2B S.KepNadilla ChoerunnisaNo ratings yet
- SE7000 Application GuideDocument102 pagesSE7000 Application GuideHujiLokoNo ratings yet
- Manage Devices & Send Photo Reports with Open Source Headwind MDMDocument7 pagesManage Devices & Send Photo Reports with Open Source Headwind MDMyasir hafeez100% (1)
- Diversity QuotasDocument7 pagesDiversity Quotasapi-609564626No ratings yet
- The Dolphin: by Sergio Bambarén. Maritza - Jhunior - Cynthia - Carlos - AlexDocument10 pagesThe Dolphin: by Sergio Bambarén. Maritza - Jhunior - Cynthia - Carlos - AlexAlexandra FlorNo ratings yet
- Elo TecDocument2 pagesElo TecMimi MimiNo ratings yet
- Ventilation Lecture 4 PH Alleen LezenDocument25 pagesVentilation Lecture 4 PH Alleen LezenNazimAhmedNo ratings yet
- CFSP Example QuestionsDocument5 pagesCFSP Example Questionsuserscribd2011No ratings yet
- 2018-06-21 Calvert County TimesDocument24 pages2018-06-21 Calvert County TimesSouthern Maryland OnlineNo ratings yet
- Advanced GeomorphologyDocument30 pagesAdvanced GeomorphologyCarlos Letras100% (3)
- Composite Fish Culture PDFDocument2 pagesComposite Fish Culture PDFHanumant JagtapNo ratings yet
- All India Test Series (2023-24)Document22 pagesAll India Test Series (2023-24)Anil KumarNo ratings yet
- Attention Deficit Hyperactivity Disorder (ADHD) in ChildrenDocument16 pagesAttention Deficit Hyperactivity Disorder (ADHD) in ChildrenVenmari Joyce Pasinos100% (1)
- Ch-19 Gas Welding, Gas Cutting & Arc WeldingDocument30 pagesCh-19 Gas Welding, Gas Cutting & Arc WeldingJAYANT KUMARNo ratings yet
- 3G3EV Installation ManualDocument55 pages3G3EV Installation ManualHajrudin SinanovićNo ratings yet
- 13 18 0038121 00 PDFDocument7 pages13 18 0038121 00 PDFRaoul JhaNo ratings yet
- Proton Pump Inhibitors v3Document5 pagesProton Pump Inhibitors v3shwampaNo ratings yet
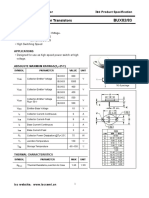
- Isc BUX82/83: Isc Silicon NPN Power TransistorsDocument2 pagesIsc BUX82/83: Isc Silicon NPN Power TransistorsCarlos HCNo ratings yet
- Rabor vs CSC - Retirement age extension disputeDocument2 pagesRabor vs CSC - Retirement age extension disputeGladys Bustria OrlinoNo ratings yet
- Test NovDocument4 pagesTest NovKatherine GonzálezNo ratings yet
- Barrioquinto vs. FernandezDocument2 pagesBarrioquinto vs. FernandezIrene RamiloNo ratings yet
- PME4 KeyDocument2 pagesPME4 KeyyazicigaamzeNo ratings yet
- Bolivia CSRDocument1 pageBolivia CSRDaniel Andrade SaavedraNo ratings yet
- Green Destination (HR Analytics)Document16 pagesGreen Destination (HR Analytics)snehal patilNo ratings yet
- CHEMIST LICENSURE EXAM TABLEDocument8 pagesCHEMIST LICENSURE EXAM TABLEJasmin NewNo ratings yet