You might also like
- Physiologic Obstetrics by APMCDocument1,091 pagesPhysiologic Obstetrics by APMCKatrina Cajigal100% (8)
- Physiological Changes During PregnancyDocument44 pagesPhysiological Changes During PregnancyvrutipatelNo ratings yet
- Myoma UteriDocument21 pagesMyoma UteriLangitBiruNo ratings yet
- WW.04.05 Contraction Stress Test (Oxytocin Challenge Test) PDFDocument3 pagesWW.04.05 Contraction Stress Test (Oxytocin Challenge Test) PDFDiah Kurniawati100% (1)
- Destructive Operations. PDFDocument63 pagesDestructive Operations. PDFFeba SajanNo ratings yet
- Definition of Contracted Pelvis and Factors Affecting LabourDocument19 pagesDefinition of Contracted Pelvis and Factors Affecting LabourAuri SururyNo ratings yet
- Antenatal Examination According To WHODocument6 pagesAntenatal Examination According To WHOManisha ThakurNo ratings yet
- 4-Drugs in Obs & GyneDocument52 pages4-Drugs in Obs & Gyneapi-37033520% (2)
- Cephalo Pelvic Disproportion (CPD) & Contracted PelvisDocument45 pagesCephalo Pelvic Disproportion (CPD) & Contracted Pelvisbinipsamuel250% (1)
- Prolonged Labor and Labor InductionDocument28 pagesProlonged Labor and Labor InductionNovia RizqiNo ratings yet
- Ectopic Pregnancy: Causes, Symptoms & TreatmentDocument10 pagesEctopic Pregnancy: Causes, Symptoms & TreatmentXo Yem0% (1)
- Vesicovaginal Fistula: Urology DepartmentDocument24 pagesVesicovaginal Fistula: Urology DepartmentHardiTariqHamma100% (1)
- Understanding Ectopic Pregnancy: Causes, Symptoms and TreatmentDocument11 pagesUnderstanding Ectopic Pregnancy: Causes, Symptoms and TreatmentPrincess BalloNo ratings yet
- Antepartum HemorrhageDocument32 pagesAntepartum HemorrhageHeskianoGoeltomNo ratings yet
- Abnormal Labor and Dystocia: Prolonged Labor, Obstructed Labor, Shoulder DystociaDocument50 pagesAbnormal Labor and Dystocia: Prolonged Labor, Obstructed Labor, Shoulder DystociaNorliana Jaafar0% (1)
- Iugr FinalDocument35 pagesIugr Finalsanthiyasandy100% (3)
- Breech PresentationDocument40 pagesBreech PresentationShuhada Wahab100% (3)
- CPD and Contracted PelvisDocument55 pagesCPD and Contracted PelvisShaells JoshiNo ratings yet
- Welcome To The Morning SessionDocument20 pagesWelcome To The Morning SessionGENERAL sharpNo ratings yet
- Polyhydramnios and OlygohydramniosDocument32 pagesPolyhydramnios and Olygohydramniosafifurrahman_rizalNo ratings yet
- Hypertensive Disorder in PregnancyDocument56 pagesHypertensive Disorder in PregnancyESCA GabrielNo ratings yet
- Prolonged Labour: Causes, Diagnosis and ManagementDocument24 pagesProlonged Labour: Causes, Diagnosis and ManagementSanthosh.S.U100% (1)
- CPD: Cephalo-Pelvic Disproportion PathophysiologyDocument3 pagesCPD: Cephalo-Pelvic Disproportion PathophysiologyTeanne Bathan100% (1)
- IugrDocument5 pagesIugrvincentsharonNo ratings yet
- History:: Obs-Gyn Antepartum HaemorrhageDocument2 pagesHistory:: Obs-Gyn Antepartum HaemorrhagejNo ratings yet
- Cephalo Pelvic DisproportionDocument43 pagesCephalo Pelvic DisproportionPabhat KumarNo ratings yet
- Puerperal Sepsis: Causes, Symptoms, PreventionDocument31 pagesPuerperal Sepsis: Causes, Symptoms, PreventionRumi Maharjan100% (1)
- Midwifery TerminologyDocument21 pagesMidwifery Terminologyelia wati100% (1)
- Induction of Labour: A Guide to Methods and ManagementDocument18 pagesInduction of Labour: A Guide to Methods and ManagementNihal ZaidiNo ratings yet
- Effects of Maternal Drugs On The FetusDocument9 pagesEffects of Maternal Drugs On The FetusJennifer DixonNo ratings yet
- Thyroid Disease in PregnancyDocument17 pagesThyroid Disease in Pregnancydaniel100% (1)
- Genital Tract InjuriesDocument37 pagesGenital Tract InjuriesShady Abdelbari83% (6)
- Forceps DeliveryDocument32 pagesForceps DeliveryVijith.V.kumar50% (2)
- Complication of PregnancyDocument55 pagesComplication of PregnancyQuolette Constante100% (1)
- Partograph DR OdofinDocument61 pagesPartograph DR OdofinEkiran BabajideNo ratings yet
- Prelabor Rupture of Membranes (Prom) : By-Aditi Grover Roll No. - 3Document12 pagesPrelabor Rupture of Membranes (Prom) : By-Aditi Grover Roll No. - 3San SiddzNo ratings yet
- HysterectomyDocument24 pagesHysterectomypt.mahmoudNo ratings yet
- TORCH in PregnancyDocument63 pagesTORCH in PregnancyKinjal VasavaNo ratings yet
- Prolong LabourDocument5 pagesProlong LabourNishaThakuri100% (1)
- Puerperal SepsisDocument34 pagesPuerperal SepsisSanthosh.S.UNo ratings yet
- Hepatitis in PregnancyDocument48 pagesHepatitis in PregnancyStanly Elliemo100% (2)
- Breast Complications in PuerperiumDocument24 pagesBreast Complications in Puerperiumvincentsharon100% (9)
- Gynaecological AssessmentDocument110 pagesGynaecological AssessmentKripa SusanNo ratings yet
- Bishop ScoreDocument5 pagesBishop ScoreJillian MendozaNo ratings yet
- AbortionsDocument99 pagesAbortionsAGERI PUSHPALATHANo ratings yet
- Ob Seminar Amniotic Fluid-1Document25 pagesOb Seminar Amniotic Fluid-1Aleena Davis100% (1)
- Gestational Trophoblastic DiseaseDocument5 pagesGestational Trophoblastic DiseaseWarshak NathNo ratings yet
- Puerperal Sepsis Causes, Symptoms, Prevention and TreatmentDocument45 pagesPuerperal Sepsis Causes, Symptoms, Prevention and TreatmentKalo kajiNo ratings yet
- MANAGEMENT OF HYDRAMNIOS AND OLIGOHYDRAMNIOSDocument12 pagesMANAGEMENT OF HYDRAMNIOS AND OLIGOHYDRAMNIOSEaster Soma HageNo ratings yet
- Vesicular MoleDocument46 pagesVesicular Moledhisazainita0% (1)
- Postpartum Hemorrhage: The First Clinical College of Three Gorges University, Wang XiaojinDocument98 pagesPostpartum Hemorrhage: The First Clinical College of Three Gorges University, Wang XiaojinMadhu Sudhan PandeyaNo ratings yet
- HysterectomyDocument2 pagesHysterectomyJellou MacNo ratings yet
- Multiple PregnancyDocument20 pagesMultiple PregnancyNurul Fahmiza TumiranNo ratings yet
- Repositioning an Inverted UterusDocument5 pagesRepositioning an Inverted Uterusshraddha vermaNo ratings yet
- Ectopic Pregnancy: DR .Urmila KarkiDocument27 pagesEctopic Pregnancy: DR .Urmila KarkiBasudev chNo ratings yet
- Normal DeliveryDocument41 pagesNormal DeliveryAliNo ratings yet
- HydramniosDocument31 pagesHydramniosSpandana DepuruNo ratings yet
- IUGRDocument11 pagesIUGRAnastasiafynnNo ratings yet
- Breech Presentation and Its Management2Document17 pagesBreech Presentation and Its Management2maezu100% (3)
- Causes and Management of Primary Uterine InertiaDocument4 pagesCauses and Management of Primary Uterine InertiaTrisha Cayabyab100% (1)
- (11-13) Assess The Knowledge On Minor Ailments of Pregnancy-FormatDocument3 pages(11-13) Assess The Knowledge On Minor Ailments of Pregnancy-FormatMudasir Ahmad BhatNo ratings yet
- Over Distension of Uterus POLYHYDRAMNIOSDocument11 pagesOver Distension of Uterus POLYHYDRAMNIOSjoel david knda mj100% (1)
- Postpartum Hemorrhage (PPH) ManagementDocument38 pagesPostpartum Hemorrhage (PPH) ManagementPrakash ThakullaNo ratings yet
- Abnormal Uterine ActionDocument36 pagesAbnormal Uterine ActionMed PoxNo ratings yet
- 1 Persiapan Penanganan Bayi Baru LahirDocument54 pages1 Persiapan Penanganan Bayi Baru LahirRosa NinmusuNo ratings yet
- Lat XiDocument3 pagesLat XiEsa NadhirNo ratings yet
- High Risk PregnanciesDocument27 pagesHigh Risk PregnanciesMochammad Adam EldiNo ratings yet
- Obstetric Coding Quality Error Trends - IPDocument36 pagesObstetric Coding Quality Error Trends - IPRavi NunavathNo ratings yet
- OB SottoDocument2 pagesOB SottoSophia VeralloNo ratings yet
- Understanding Molar Pregnancy and Gestational Trophoblastic DiseaseDocument55 pagesUnderstanding Molar Pregnancy and Gestational Trophoblastic DiseaseClarains FriskaNo ratings yet
- Tutorial 3 APH, PP, VP, AbruptioDocument55 pagesTutorial 3 APH, PP, VP, AbruptioBahirahNo ratings yet
- M1 Post Task - Caparas-Bsn2a-A2Document2 pagesM1 Post Task - Caparas-Bsn2a-A2Gretta CaparasNo ratings yet
- Management of Early Onset FGR - A. BaschatDocument4 pagesManagement of Early Onset FGR - A. BaschatLokesh KhuranaNo ratings yet
- The Grand MultiparaDocument5 pagesThe Grand MultiparaIndhumathiNo ratings yet
- High Risk of PregnancyDocument16 pagesHigh Risk of PregnancyGeraldine PatayanNo ratings yet
- Individual Activity #3: CHAPTER STUDY QUESTIONS: Rubric For Short AnswerDocument11 pagesIndividual Activity #3: CHAPTER STUDY QUESTIONS: Rubric For Short AnswerSatanichia McDowell KurumizawaNo ratings yet
- Jurnal Wedang Jahe Terhadap Emesis GravidarumDocument6 pagesJurnal Wedang Jahe Terhadap Emesis GravidarumRetiAstiraNo ratings yet
- A Prelim CAMCARDocument18 pagesA Prelim CAMCARIvan VillapandoNo ratings yet
- Jurnal KesehatanDocument24 pagesJurnal KesehatanNabila AzzaetunaNo ratings yet
- Cord ProlapseDocument3 pagesCord ProlapseNise Mon KuriakoseNo ratings yet
- RH Isoimmunization (PritDocument23 pagesRH Isoimmunization (PritmaezuNo ratings yet
- High Risk PregnancyDocument35 pagesHigh Risk PregnancykenNo ratings yet
- CMCA ASSIGNMENT #1b PDFDocument3 pagesCMCA ASSIGNMENT #1b PDFAyanami PascuaNo ratings yet
- Q.P. Code: 641375Document7 pagesQ.P. Code: 641375Mani RuzzamanNo ratings yet
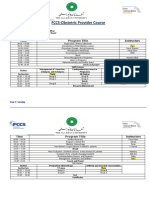
- FCCS-Obstetric Provider Course: Time Program Title InstructorsDocument2 pagesFCCS-Obstetric Provider Course: Time Program Title InstructorsSamina AyazNo ratings yet
- Nursing Exam Questions on Maternal and Newborn CareDocument25 pagesNursing Exam Questions on Maternal and Newborn CareRex PaulrajNo ratings yet
- Jurnal MeiristaDocument8 pagesJurnal Meiristameirista deviNo ratings yet
- Hubungan Psikologis Ibu Hamil Dengan Kejadian Hiperemesis GravidarumDocument6 pagesHubungan Psikologis Ibu Hamil Dengan Kejadian Hiperemesis GravidarumAlfaridziNo ratings yet
- Emergency Childbirth ProtocolDocument3 pagesEmergency Childbirth ProtocolKenneth DizonNo ratings yet