You might also like
- Anam FinalDocument82 pagesAnam FinalHussain AzharNo ratings yet
- K HomeosDocument47 pagesK HomeosHussain AzharNo ratings yet
- Ion SyndromeDocument67 pagesIon SyndromeHussain AzharNo ratings yet
- Electrolyte Disturbaces - Hyponatremia and HypernatremiaDocument41 pagesElectrolyte Disturbaces - Hyponatremia and HypernatremiaMohammad AliNo ratings yet
- Enteric FeverDocument63 pagesEnteric FeverHussain AzharNo ratings yet
- Liver Function Test FinalDocument98 pagesLiver Function Test FinalHussain AzharNo ratings yet
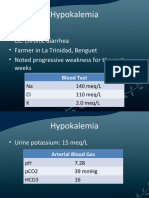
- HypokalemiaDocument12 pagesHypokalemiaMohammad AliNo ratings yet
- DVT - 2 FaizaDocument65 pagesDVT - 2 FaizaHussain AzharNo ratings yet
- Case Presentation 2Document53 pagesCase Presentation 2Hussain AzharNo ratings yet
- DVT&PE Final 1Document59 pagesDVT&PE Final 1Hussain AzharNo ratings yet
- EFFA PRESENTATNhepatic EncephalopathyDocument50 pagesEFFA PRESENTATNhepatic EncephalopathyHussain AzharNo ratings yet
- CP Najma 97Document75 pagesCP Najma 97Hussain AzharNo ratings yet
- DKA Concepts and ManagementDocument22 pagesDKA Concepts and ManagementMohammad AliNo ratings yet
- DVTDocument32 pagesDVTHussain AzharNo ratings yet
- Dka 31-05-11Document52 pagesDka 31-05-11Hussain AzharNo ratings yet
- AntibioticsDocument49 pagesAntibioticsHussain AzharNo ratings yet
- Dengue 2009Document53 pagesDengue 2009Hussain AzharNo ratings yet
- Case Presentation ParaplegiaDocument51 pagesCase Presentation ParaplegiaHussain Azhar100% (2)
- Acute Renal FailureDocument120 pagesAcute Renal FailureHussain AzharNo ratings yet
- Case Presentation Hypokalemic ManDocument61 pagesCase Presentation Hypokalemic ManHussain AzharNo ratings yet
- Asthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueDocument47 pagesAsthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueMohammad AliNo ratings yet
- Acrf CDocument70 pagesAcrf CHussain AzharNo ratings yet
- AKIDocument83 pagesAKIHussain AzharNo ratings yet
- Approach To Unconsious PTDocument62 pagesApproach To Unconsious PTHussain AzharNo ratings yet
- AnemiaDocument37 pagesAnemiaHussain AzharNo ratings yet
- An Approach To Anemic PatientDocument79 pagesAn Approach To Anemic PatientHussain AzharNo ratings yet
- Dr. Adeel Ahmed Waheed: House Officer M-4Document84 pagesDr. Adeel Ahmed Waheed: House Officer M-4Hussain AzharNo ratings yet
- ABG S Final and Last TouchDocument88 pagesABG S Final and Last TouchHussain AzharNo ratings yet
- Acute Exacerbation of COPDDocument14 pagesAcute Exacerbation of COPDMohammad AliNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Vyntus-CPX BR EN PDFDocument8 pagesVyntus-CPX BR EN PDFLajoskaNo ratings yet
- Brigham 2019 MCQsDocument13 pagesBrigham 2019 MCQsfarex100% (1)
- Chronic Cough - Diagnosis and Treatment - Mayo ClinicDocument11 pagesChronic Cough - Diagnosis and Treatment - Mayo ClinicMUNIRAH SUHAIBAH BINTI SULAIMAN STUDENTNo ratings yet
- 'COMPREHENSIVE SOLUTIONS' Combi - Dr. Afsar Khan PDFDocument587 pages'COMPREHENSIVE SOLUTIONS' Combi - Dr. Afsar Khan PDFwattuser KassoNo ratings yet
- 2019 Nutrition in Cystic Fibrosis - From The Past To The Present and Into The FutureDocument18 pages2019 Nutrition in Cystic Fibrosis - From The Past To The Present and Into The FutureMaria Paula CastroNo ratings yet
- Drager Carina GuideDocument24 pagesDrager Carina Guidengocbienk5650% (2)
- Manual Maquina de Anestesia Mindray A5Document244 pagesManual Maquina de Anestesia Mindray A5camila cubidesNo ratings yet
- Bmi-2 MarksDocument16 pagesBmi-2 MarksmohanapriyaNo ratings yet
- Penlon AV-S - Technical Training Course PDFDocument174 pagesPenlon AV-S - Technical Training Course PDFluisNo ratings yet
- Topic 2 COPD and AsthmaDocument18 pagesTopic 2 COPD and AsthmaCaitlynNo ratings yet
- TSRA Review of Cardiothoracic PDFDocument298 pagesTSRA Review of Cardiothoracic PDFvamshidhNo ratings yet
- Effect of Bhastrika Pranayama and Exercise On Lung.1655Document2 pagesEffect of Bhastrika Pranayama and Exercise On Lung.1655Adrian ScurtuNo ratings yet
- Azithromycin For Acute Exacerbations of Asthma The AZALEA Randomized Clinical TrialDocument8 pagesAzithromycin For Acute Exacerbations of Asthma The AZALEA Randomized Clinical TrialicaeeeNo ratings yet
- Inspiratory Muscle TrainingDocument16 pagesInspiratory Muscle Trainingtim0workmanNo ratings yet
- 2012 100 Cases in Radiology (2012) - 1Document321 pages2012 100 Cases in Radiology (2012) - 1Gabriel SantosNo ratings yet
- LECTURE NOTE ON ASTHMA-WPS OfficeDocument7 pagesLECTURE NOTE ON ASTHMA-WPS OfficeNaija Nurses TVNo ratings yet
- Jurnal ParuDocument10 pagesJurnal ParuRia RioNo ratings yet
- MIR Spirolab 2 - User ManualDocument46 pagesMIR Spirolab 2 - User Manualroberto.aNo ratings yet
- Carescape R860: Participant GuideDocument142 pagesCarescape R860: Participant GuideМаксим МатяшNo ratings yet
- AsthmaDocument57 pagesAsthmaVladanNo ratings yet
- Pulmonary Function Testing ExplainedDocument42 pagesPulmonary Function Testing ExplainedIulia DNo ratings yet
- Examination of The Chest and LungsDocument5 pagesExamination of The Chest and Lungsteena12aNo ratings yet
- Respiratory Therapists Licensure Exam GuideDocument21 pagesRespiratory Therapists Licensure Exam GuideCPD MASNo ratings yet
- Kunioer Mini AqlqDocument7 pagesKunioer Mini AqlqMafia 12mia5No ratings yet
- COPD Indian GuidelinesDocument64 pagesCOPD Indian GuidelinesNitesh GuptaNo ratings yet
- PhysioEx Exercise 7 Activity 2Document8 pagesPhysioEx Exercise 7 Activity 2villanuevaparedesaracely4No ratings yet
- Ats Efr 2023Document75 pagesAts Efr 2023MarcelaNo ratings yet
- Eucalyptol (1,8-Cineole) : An Underutilized Ally in Respiratory Disorders?Document9 pagesEucalyptol (1,8-Cineole) : An Underutilized Ally in Respiratory Disorders?Koko “urya” No NekoNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument16 pagesChronic Obstructive Pulmonary DiseaseAlberto MedinaNo ratings yet
- COPD Risk Factors & Spirometry StagingDocument38 pagesCOPD Risk Factors & Spirometry StagingKudingLimMingYaoNo ratings yet