You might also like
- GalactosemiaDocument3 pagesGalactosemianyx001No ratings yet
- Galactosemia by Group 9Document41 pagesGalactosemia by Group 9Sree Balaji Srinivas Katakam100% (1)
- Maternal PhysiologyDocument43 pagesMaternal PhysiologyRaiza Love Caparas-PablicoNo ratings yet
- Clinical Presentation and Diagnosis of Tuberculosis: International Standards 1-5Document51 pagesClinical Presentation and Diagnosis of Tuberculosis: International Standards 1-5Gilbert Solomon TantonoNo ratings yet
- Group 6-B2 - Telomerase, Aging and CancerDocument76 pagesGroup 6-B2 - Telomerase, Aging and CancerJohn Michael Vicente100% (1)
- Pku AlkDocument33 pagesPku AlkSharf WangNo ratings yet
- 05 - Sle, DMZ, PHSDocument157 pages05 - Sle, DMZ, PHSG SNo ratings yet
- Protein Malnutrition: Understanding Kwashiorkor and MarasmusDocument19 pagesProtein Malnutrition: Understanding Kwashiorkor and MarasmusJanine Kristine ManaoisNo ratings yet
- Marasmus - Case ReportDocument13 pagesMarasmus - Case ReportApriany Cordias Arlita SilalahiNo ratings yet
- Understanding Malnutrition: Marasmus, Kwashiorkor and TreatmentDocument23 pagesUnderstanding Malnutrition: Marasmus, Kwashiorkor and TreatmentBashar KhalilNo ratings yet
- Systemic Carnitine Deficiency: Causes, Symptoms and TreatmentDocument27 pagesSystemic Carnitine Deficiency: Causes, Symptoms and TreatmentALSiyNo ratings yet
- Nutritional Deficiency Disorder/ (PEM)Document37 pagesNutritional Deficiency Disorder/ (PEM)ShrutiNo ratings yet
- Explain The Ff. Manifestations in The Different Cases That Are Discused BelowDocument29 pagesExplain The Ff. Manifestations in The Different Cases That Are Discused BelowRodel Paulo Tangunan GarciaNo ratings yet
- NSAIDDocument15 pagesNSAIDMaria KhawajaNo ratings yet
- Hemorrhagic Disease of The NewbornDocument3 pagesHemorrhagic Disease of The NewbornDevi SuryandariNo ratings yet
- Nephrotic Syndrome 2016Document45 pagesNephrotic Syndrome 2016alaaNo ratings yet
- Nephrotic Syndrome: Jaiganesh.M, M.D (General Medicine) Asst. Professor, S.M.C.HDocument60 pagesNephrotic Syndrome: Jaiganesh.M, M.D (General Medicine) Asst. Professor, S.M.C.HJaiganesh MuruganandamNo ratings yet
- Protozoan Parasites Causing Malaria, Sleeping Sickness, Leishmaniasis and MoreDocument32 pagesProtozoan Parasites Causing Malaria, Sleeping Sickness, Leishmaniasis and MoreFort SalvadorNo ratings yet
- Cell Injury Pathology Chapter 01 NotesDocument6 pagesCell Injury Pathology Chapter 01 NotesAmeerHamzaNo ratings yet
- Hematology & Immune SystemDocument81 pagesHematology & Immune SystemAmanuel Maru100% (1)
- Metabolic Disorders GuideDocument80 pagesMetabolic Disorders GuideXeniyaFedoryakNo ratings yet
- Medical Diseases Complicating Pregnancy: by The Name of AllahDocument45 pagesMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيNo ratings yet
- Clinical EnzymologyDocument25 pagesClinical Enzymologyaminata6No ratings yet
- Nitrogen Metabolism: Nitrate AssimilationDocument3 pagesNitrogen Metabolism: Nitrate AssimilationSalsabila LuqyanaNo ratings yet
- AtherosclerosisDocument14 pagesAtherosclerosisDeepak Raj100% (1)
- RBC Disorder BcqsDocument68 pagesRBC Disorder BcqsMukhtiar AhmedNo ratings yet
- Stroke IskemikDocument237 pagesStroke IskemikVania ValentinaNo ratings yet
- Clinical Examination of Genitourinary SystemDocument43 pagesClinical Examination of Genitourinary SystemKeamina .aNo ratings yet
- Approach to pediatric anemia diagnosis and classificationDocument18 pagesApproach to pediatric anemia diagnosis and classificationMade Oka HeryanaNo ratings yet
- Tropical Splenomegaly SyndromeDocument12 pagesTropical Splenomegaly SyndromeSaidAandySaida100% (1)
- Fetal Growth Restriction - ACOG 2019Document23 pagesFetal Growth Restriction - ACOG 2019Adhitya Yudha MaulanaNo ratings yet
- FAT Soluble VitaminsDocument53 pagesFAT Soluble VitaminsFaria LatifNo ratings yet
- Acute Kidney InjuryDocument21 pagesAcute Kidney InjuryAtif Gazali100% (1)
- Drug Heart Failure MDocument24 pagesDrug Heart Failure MAthari KhanNo ratings yet
- Paediatric Diabetic KetoacidosisDocument7 pagesPaediatric Diabetic KetoacidosisJuan Carlos BayonaNo ratings yet
- JaundiceDocument4 pagesJaundiceAbo Omar Ahmed100% (1)
- DIABETIC COMA - Clinical Features and ManagementDocument54 pagesDIABETIC COMA - Clinical Features and ManagementRitesh SinghNo ratings yet
- SepsisDocument33 pagesSepsisv_vijayakanth7656No ratings yet
- Glaucoma Diagnosis & Treatment GuideDocument42 pagesGlaucoma Diagnosis & Treatment GuideSaha DirllahNo ratings yet
- Thalassemias and HemoglobinopathiesDocument63 pagesThalassemias and HemoglobinopathiesMahmod_Al_Bust_4830No ratings yet
- Hypo Album inDocument11 pagesHypo Album inAndi Agung RiatmojoNo ratings yet
- 13 - Surgical InfectionsDocument26 pages13 - Surgical InfectionsEma KhalilNo ratings yet
- Liver TransplantDocument3 pagesLiver Transplantsamitbisen0% (1)
- Osh State UniversityDocument14 pagesOsh State Universitykhuzaima9No ratings yet
- Hepatic Failure & Hepatic EncephalopathyDocument37 pagesHepatic Failure & Hepatic Encephalopathyapi-19916399No ratings yet
- Endang Windiastuti Division of Hematology-Oncology Department of Child Health DR Cipto Mangunkusumo Hospital, FMUIDocument27 pagesEndang Windiastuti Division of Hematology-Oncology Department of Child Health DR Cipto Mangunkusumo Hospital, FMUIAnonymous NRDU0bLFSNo ratings yet
- Urolithiasis: ObjectivesDocument11 pagesUrolithiasis: ObjectivesOkki Masitah Syahfitri NasutionNo ratings yet
- Electromyography I PDFDocument13 pagesElectromyography I PDFkeithtrahNo ratings yet
- Management of Lymphomas: 2018 Indian Expert ConsensusDocument24 pagesManagement of Lymphomas: 2018 Indian Expert ConsensusAndi SusiloNo ratings yet
- Diabetes MellitusDocument17 pagesDiabetes MellitusRuqayya KobatteNo ratings yet
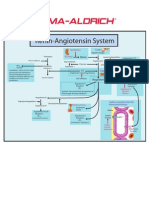
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Pyelonephritis: Dr. Shraddha Koirala Department of Pathology NMCTHDocument26 pagesPyelonephritis: Dr. Shraddha Koirala Department of Pathology NMCTHUrusha MagarNo ratings yet
- Imuune Thrombocytopenia (Itp)Document34 pagesImuune Thrombocytopenia (Itp)Roshandiep GillNo ratings yet
- Congenital SyphilisDocument6 pagesCongenital SyphilisFrozen Pandora MahayaNo ratings yet
- Fetal MembranesDocument17 pagesFetal MembranesQaiser InayatNo ratings yet
- CNS Congenital AnomaliesDocument74 pagesCNS Congenital AnomaliesMoh DrhusseinyNo ratings yet
- Hepatic EncephalopathyDocument21 pagesHepatic EncephalopathyAnonymous n3qy0JdCgNo ratings yet
- Dental Diabetes ManagementDocument30 pagesDental Diabetes ManagementChitrang KolawaleNo ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Digestive System PowerpointDocument33 pagesDigestive System PowerpointThomas41767% (6)
- Confidence Intervals For Ratio of Two Poisson Rates Using The Method of Variance Estimates RecoveryDocument23 pagesConfidence Intervals For Ratio of Two Poisson Rates Using The Method of Variance Estimates RecoveryJaneNo ratings yet
- Week 4-Physical Fitness TestDocument38 pagesWeek 4-Physical Fitness TestCatherine Sagario OliquinoNo ratings yet
- Personality Disorders Cluster CDocument19 pagesPersonality Disorders Cluster CPahw BaluisNo ratings yet
- ASP ProductsDocument33 pagesASP ProductsSerghei Barba100% (1)
- Family Nursing Care PlanDocument1 pageFamily Nursing Care PlanDersly LaneNo ratings yet
- HSE List of PublicationsDocument12 pagesHSE List of PublicationsDanijel PindrićNo ratings yet
- TULUA Lipoabdominoplasty Transversal Aponeurotic.12Document14 pagesTULUA Lipoabdominoplasty Transversal Aponeurotic.12Carolina Ormaza Giraldo100% (1)
- Heart Failure Lily ModifiedDocument57 pagesHeart Failure Lily ModifiedSabila FatimahNo ratings yet
- Liquefied Gas Tanker Familiarisation Course: Operational & Support LevelDocument60 pagesLiquefied Gas Tanker Familiarisation Course: Operational & Support LevelAlpha OmegaNo ratings yet
- RNTCP - Wikipedia, The Free EncyclopediaDocument5 pagesRNTCP - Wikipedia, The Free EncyclopediaakurilNo ratings yet
- Jha For Painting of EquipmentDocument1 pageJha For Painting of EquipmentShahid RazaNo ratings yet
- Congenital LaryngomalaciaDocument8 pagesCongenital LaryngomalaciaRettha SigiroNo ratings yet
- Family Case AnalysisDocument194 pagesFamily Case AnalysisDianneNo ratings yet
- MDR Guideline Medical Devices LabelingDocument7 pagesMDR Guideline Medical Devices Labelingarade43100% (1)
- Immunology Serology Blood BankingDocument5 pagesImmunology Serology Blood BankingEdsss Villar100% (3)
- Symbols On PackegingDocument3 pagesSymbols On PackegingsakibarsNo ratings yet
- Pneumonia Care PlanDocument1 pagePneumonia Care Plantcumurphish67% (3)
- 100-Bed General Hospital LayoutDocument1 page100-Bed General Hospital LayoutAshish chauhanNo ratings yet
- Topical Agents and Dressings For Local Burn Wound CareDocument25 pagesTopical Agents and Dressings For Local Burn Wound CareViresh Upase Roll No 130. / 8th termNo ratings yet
- Informed Consent and Release, Waiver, and Quitclaim: Know All Men by These PresentsDocument2 pagesInformed Consent and Release, Waiver, and Quitclaim: Know All Men by These PresentsRobee Camille Desabelle-SumatraNo ratings yet
- Abbott Rabeprazole PM e PDFDocument45 pagesAbbott Rabeprazole PM e PDFdonobacaNo ratings yet
- Breakfast of ChampionsDocument34 pagesBreakfast of ChampionsTamanna TabassumNo ratings yet
- Jordan Leavy Carter Criminal ComplaintDocument10 pagesJordan Leavy Carter Criminal ComplaintFOX 11 NewsNo ratings yet
- Methodological Literature Review 1 1Document8 pagesMethodological Literature Review 1 1api-584018105No ratings yet
- Clinical Biomechanics in Implant DentistryDocument36 pagesClinical Biomechanics in Implant DentistryMahadevan Ravichandran100% (4)
- Post MortemDocument4 pagesPost MortemErlinda YulyNo ratings yet
- Journal Homepage: - : IntroductionDocument3 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Psychoeducational and Family Therapy in Relapse PreventionDocument4 pagesPsychoeducational and Family Therapy in Relapse PreventionEdson HilárioNo ratings yet