You might also like
- Depression Medications ExplainedDocument5 pagesDepression Medications ExplainedxyzNo ratings yet
- ANTIDEPRESSANT DRUGS: Types, Mechanisms and Side EffectsDocument21 pagesANTIDEPRESSANT DRUGS: Types, Mechanisms and Side EffectsKashis SharmaNo ratings yet
- AntidepressantsDocument5 pagesAntidepressantsUm HamoOd100% (2)
- Psychopharmacology in Psychiatry: Neurotransmitter Pharmacology and Drug MechanismsDocument77 pagesPsychopharmacology in Psychiatry: Neurotransmitter Pharmacology and Drug MechanismschachaazkaNo ratings yet
- Anti PsychoticsDocument34 pagesAnti Psychotics88AKKNo ratings yet
- The Maudsley Prescribing Guidelines in PsychiatryFrom EverandThe Maudsley Prescribing Guidelines in PsychiatryRating: 5 out of 5 stars5/5 (1)
- Current Clinical Strategies: Handbook of Psychiatric DrugsDocument72 pagesCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116No ratings yet
- Understanding Schizoaffective DisorderDocument2 pagesUnderstanding Schizoaffective DisorderRumana AliNo ratings yet
- CNS StimulantDocument26 pagesCNS StimulantIslam Abdo50% (2)
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDocument29 pagesPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaNo ratings yet
- Overview of Psychotropic DrugsDocument7 pagesOverview of Psychotropic Drugsnad101No ratings yet
- Anidepressant Drugs: Pratik KhanalDocument37 pagesAnidepressant Drugs: Pratik KhanalPratik Khanal100% (1)
- Sedative HypnoticsDocument41 pagesSedative HypnoticsPatrick Juacalla100% (2)
- Pharmacology and Toxicology of Antidepressants and AntipsychoticsDocument50 pagesPharmacology and Toxicology of Antidepressants and AntipsychoticsPintu Bhushan MitraNo ratings yet
- Treatment Modalities For Mood DisordersDocument55 pagesTreatment Modalities For Mood DisordersGlory MimiNo ratings yet
- B /G C U I R: Anti-PsychoticsDocument2 pagesB /G C U I R: Anti-PsychoticsErsy Sakti ilhamNo ratings yet
- Psychoses: CNS Dopamine Levels Perception, Thought, Consciousness, Social, Affective DisordersDocument3 pagesPsychoses: CNS Dopamine Levels Perception, Thought, Consciousness, Social, Affective DisordersJustin Hulin100% (1)
- AntiemeticsDocument25 pagesAntiemeticsPridho GaziansyahNo ratings yet
- Mental Health and Psychiatric Nursing: Vernalin B. Terrado, RNDocument35 pagesMental Health and Psychiatric Nursing: Vernalin B. Terrado, RNverna100% (1)
- Anxiety Disorders: Types, Symptoms, and TreatmentsDocument62 pagesAnxiety Disorders: Types, Symptoms, and TreatmentsPRHSTNo ratings yet
- INTRODUCTION TO NEUROPHARMACOLOGYyyDocument27 pagesINTRODUCTION TO NEUROPHARMACOLOGYyyEbad RazviNo ratings yet
- Antidepressant Pharmacology: TCAs, SSRIs and Mechanisms of ActionDocument3 pagesAntidepressant Pharmacology: TCAs, SSRIs and Mechanisms of ActionThư Phạm100% (1)
- Table 1: Substrates of Cytochrome P450 (CYP) EnzymesDocument6 pagesTable 1: Substrates of Cytochrome P450 (CYP) EnzymesNurul Kamilah SadliNo ratings yet
- AntidepressantsDocument59 pagesAntidepressantsanon_189054600100% (2)
- Antidepressant Therapy AlgorithmDocument12 pagesAntidepressant Therapy AlgorithmZubair Mahmood KamalNo ratings yet
- Atypical Antidepressants - Pharmacology, Administration, and Side Effects - UpToDateDocument16 pagesAtypical Antidepressants - Pharmacology, Administration, and Side Effects - UpToDateMelissandreNo ratings yet
- 03.1A PsychopharmacologyDocument160 pages03.1A PsychopharmacologyJoe BloggsNo ratings yet
- Pharmacology of Movement DisordersDocument4 pagesPharmacology of Movement DisordersjslumNo ratings yet
- Pediatrics: St. Elizabeth Family Medicine Residency ProgramDocument9 pagesPediatrics: St. Elizabeth Family Medicine Residency Programwingchun108tekNo ratings yet
- Examples: Inability To Sit Still, Pacing, Wringing of Hands, or Pulling of ClothingDocument14 pagesExamples: Inability To Sit Still, Pacing, Wringing of Hands, or Pulling of ClothingFaith Dianasas RequinaNo ratings yet
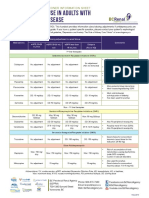
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Psycho PharmaDocument8 pagesPsycho PharmaMark JosephNo ratings yet
- Psychopharmacology 1Document7 pagesPsychopharmacology 1RajP01No ratings yet
- Pharmacotherapy in PschiatryDocument8 pagesPharmacotherapy in PschiatryygfhdgNo ratings yet
- PsychopharmacologyDocument31 pagesPsychopharmacologyCon BernardinoNo ratings yet
- LECTURE 22: Antipsychotic Agents & Lithium: OutlineDocument5 pagesLECTURE 22: Antipsychotic Agents & Lithium: OutlineRosa PalconitNo ratings yet
- Introduction To NeuropharmacologyDocument6 pagesIntroduction To Neuropharmacologyammarhafez78100% (1)
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDocument6 pagesAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord VerazonNo ratings yet
- Module 1 - IntroductionDocument30 pagesModule 1 - Introductionpsychopharmacology100% (2)
- Revellionz'19 - Second Year Question BankDocument114 pagesRevellionz'19 - Second Year Question BankRamNo ratings yet
- Gout DrugsDocument1 pageGout DrugsMichael BrownNo ratings yet
- Anxiety Disorders Treatment OptionsDocument5 pagesAnxiety Disorders Treatment OptionsJohn HolmesNo ratings yet
- Dr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityDocument41 pagesDr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityredderdatNo ratings yet
- Third Generation Antipsychotic DrugsDocument45 pagesThird Generation Antipsychotic DrugsGabriela Drima100% (1)
- Biological Bases Study GuideDocument13 pagesBiological Bases Study Guideapi-421695293No ratings yet
- Psychotropic Medications: Dale Sanderson, PA-C Physician Assistant Seattle Mental HealthDocument72 pagesPsychotropic Medications: Dale Sanderson, PA-C Physician Assistant Seattle Mental HealthMichael Urrutia100% (2)
- Geriatric Giants - DR SeymourDocument108 pagesGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Drugs For NeurolepticsDocument1 pageDrugs For Neurolepticssyamil_daudNo ratings yet
- Major P450 Isoforms and Their Inducers and InhibitorsDocument1 pageMajor P450 Isoforms and Their Inducers and InhibitorsM. JoyceNo ratings yet
- Side Effects of Anti Psychotic MedicationsDocument11 pagesSide Effects of Anti Psychotic MedicationsluciapopNo ratings yet
- (OS 213) LEC 03 Drugs Acting On The Respiratory System (1) - 1Document16 pages(OS 213) LEC 03 Drugs Acting On The Respiratory System (1) - 1Yavuz DanisNo ratings yet
- Shortened REM Latency and Increased REM: Previous AttemptDocument19 pagesShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenNo ratings yet
- Drug List Psych Optho NeuroDocument22 pagesDrug List Psych Optho NeuroAshley BarrileNo ratings yet
- Antidepressants Comparison Guide Most Commonly Prescribed: Recommend GenericsDocument3 pagesAntidepressants Comparison Guide Most Commonly Prescribed: Recommend GenericsCarina ColtuneacNo ratings yet
- Antidepressant AgentsDocument38 pagesAntidepressant AgentsdidiNo ratings yet
- Antipsychotics Guide for Nursing Intervention and Patient EducationDocument10 pagesAntipsychotics Guide for Nursing Intervention and Patient Educationwawing16No ratings yet
- Substance Use DisordersDocument28 pagesSubstance Use DisordersAbdul NazarNo ratings yet
- Ketamine For Opiate WithdrawalDocument3 pagesKetamine For Opiate WithdrawalroboNo ratings yet
- Pharmacology Medical Suffixes Cheat SheetDocument1 pagePharmacology Medical Suffixes Cheat SheetPattyNo ratings yet
- Second and Third Generation Antipsychotics: A Comprehensive HandbookFrom EverandSecond and Third Generation Antipsychotics: A Comprehensive HandbookRating: 5 out of 5 stars5/5 (1)
- Classification Des MédicamentsDocument28 pagesClassification Des MédicamentsGustyl KolinsNo ratings yet
- Products List of MegaDocument2 pagesProducts List of MegaIbrahima TraoreNo ratings yet
- New Materi Pretest Skill Blok 10Document3 pagesNew Materi Pretest Skill Blok 10asabri yunisNo ratings yet
- Drug Tests User Guide NEWDocument16 pagesDrug Tests User Guide NEWzxcv1ingrNo ratings yet
- Marikina Drug Symposium Highlights Dangers of Shabu, Marijuana and InhalantsDocument2 pagesMarikina Drug Symposium Highlights Dangers of Shabu, Marijuana and InhalantsLoeyNo ratings yet
- Atc DDD Tablet Buat Pa IjalDocument57 pagesAtc DDD Tablet Buat Pa IjalAriesta PerwitasariNo ratings yet
- Missed questions on drugs and alcoholDocument4 pagesMissed questions on drugs and alcoholmelodyfathiNo ratings yet
- Label ObatDocument14 pagesLabel Obatfaisal abdaNo ratings yet
- GTU BPharm Pharmacology 1 Exam QuestionsDocument8 pagesGTU BPharm Pharmacology 1 Exam QuestionsMaharshi PandyaNo ratings yet
- How the penis achieves erectionDocument5 pagesHow the penis achieves erectionMohammad Asim AnsariNo ratings yet
- SinonimDocument3 pagesSinonimindah indahNo ratings yet
- Psychiatry Pharmacology J. Psychiatry' AntidepressantsDocument9 pagesPsychiatry Pharmacology J. Psychiatry' AntidepressantssumithjalyNo ratings yet
- Bukti Pelaksanaan Obat Lasa Dan High AlertDocument12 pagesBukti Pelaksanaan Obat Lasa Dan High AlertTut RaiNo ratings yet
- Top 200 DrugsDocument9 pagesTop 200 DrugsSachin KumarNo ratings yet
- Whole Pharmacology Classification: Adrenergic Antagonists Alpha Adrenergic Antagonists Alpha 1 AntagonistsDocument17 pagesWhole Pharmacology Classification: Adrenergic Antagonists Alpha Adrenergic Antagonists Alpha 1 AntagonistsFlorina TrutescuNo ratings yet
- Doctors Opinion UPDATEDDocument3 pagesDoctors Opinion UPDATEDgpaul44No ratings yet
- 4 - St. Mary's - December 2020 AdmissionDocument100 pages4 - St. Mary's - December 2020 AdmissionprashantNo ratings yet
- Sketchy PharmDocument7 pagesSketchy PharmKacie Jo DillowNo ratings yet
- Types of Drugs and Their EffectsDocument16 pagesTypes of Drugs and Their EffectsLynbert AntoneNo ratings yet
- Drugs Affecting The Central Nervous SystemDocument16 pagesDrugs Affecting The Central Nervous SystemShafaqNo ratings yet
- Laporan Fornas Non FornasDocument6 pagesLaporan Fornas Non FornasrestyNo ratings yet
- Rekap Penerimaan Obat E-KatalogDocument39 pagesRekap Penerimaan Obat E-KatalogSantyNo ratings yet
- Phentermine 37.5 MGDocument4 pagesPhentermine 37.5 MGMichealNo ratings yet
- Drug Addiction Project ReportDocument24 pagesDrug Addiction Project ReportLohit Das100% (1)
- Monthly Report on Tablet, Syrup, Ointment/Eye Drops, and Injection MedicinesDocument9 pagesMonthly Report on Tablet, Syrup, Ointment/Eye Drops, and Injection MedicinesYulya MayasaryNo ratings yet
- (CL15) Cholinergic and Anticholinergic Agentscholinergic and Anticholinergic Agents - ImaDocument41 pages(CL15) Cholinergic and Anticholinergic Agentscholinergic and Anticholinergic Agents - ImaRahman Anwar100% (1)
- GA Dengan Intubasi EndotrachealDocument21 pagesGA Dengan Intubasi EndotrachealMuhammad Nur AlamsyahNo ratings yet
- Stok 4 Maret 2022Document40 pagesStok 4 Maret 2022dr anggaNo ratings yet
- Anti Adrenergic Drugs ArpanDocument8 pagesAnti Adrenergic Drugs ArpanA2Z GyanNo ratings yet
- Cannabinoid Boiling Points THC CBD - 0 PDFDocument1 pageCannabinoid Boiling Points THC CBD - 0 PDFmagiqoNo ratings yet