You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Export Act 1963Document27 pagesExport Act 1963Anonymous OPix6Tyk5INo ratings yet
- ENT Atlas Web PDFDocument442 pagesENT Atlas Web PDFIsabella CrăciunNo ratings yet
- Cross Taping - A Practical Guide 12Document2 pagesCross Taping - A Practical Guide 12jfjjfjfjjfjfNo ratings yet
- Free Class Asclepio Metabolic SyndromeDocument6 pagesFree Class Asclepio Metabolic SyndromeJames BudiantoNo ratings yet
- Stacey Luneke ResearchfinalDocument9 pagesStacey Luneke Researchfinalapi-309088550No ratings yet
- Paper - B Written Test Paper For Selection of Teachers: CSB 2013 English (PGT) : Subject Code: P11Document4 pagesPaper - B Written Test Paper For Selection of Teachers: CSB 2013 English (PGT) : Subject Code: P11Amrit SinhaNo ratings yet
- Palliative Care Pain and Symptom Control GuidelinesDocument128 pagesPalliative Care Pain and Symptom Control GuidelinesAQSA AHMED SIDDIQUINo ratings yet
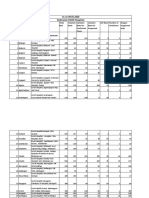
- Nairobi Morbidity 1st Qrt-2010-11Document49 pagesNairobi Morbidity 1st Qrt-2010-11Dominic KikuyuNo ratings yet
- Hiddensee - Michelle HartDocument13 pagesHiddensee - Michelle HartviniciuscarpeNo ratings yet
- FinalDocument3 pagesFinalAnupam Saraf IINo ratings yet
- Ozomed BrochureDocument4 pagesOzomed BrochurechirakiNo ratings yet
- Gynae-L - MukundaDocument50 pagesGynae-L - MukundadocivirusNo ratings yet
- Nursing Care For BipolarDocument3 pagesNursing Care For BipolarAnthonyChapotin100% (2)
- List COVID Facilities State OdishaDocument3 pagesList COVID Facilities State OdishadrjyotivetNo ratings yet
- Struggle and Survival of Native Americans: A Study in Selected Poems by Simon J. OrtizDocument15 pagesStruggle and Survival of Native Americans: A Study in Selected Poems by Simon J. OrtizCycilian ArmandoNo ratings yet
- Target Product Profile Imbruvica - IbrutinibDocument1 pageTarget Product Profile Imbruvica - IbrutinibDiti ShahNo ratings yet
- Scheme of Instruction IIScDocument236 pagesScheme of Instruction IIScRS1678No ratings yet
- Digestive System Disorder NCLEX Practice QuizDocument7 pagesDigestive System Disorder NCLEX Practice Quizjules100% (1)
- Effect of Dragon Fruit On Lipid ProfileDocument2 pagesEffect of Dragon Fruit On Lipid ProfileElindah Ayunin ArrumNo ratings yet
- Msds ChosunDocument6 pagesMsds ChosunDheeraj E MohananNo ratings yet
- Acute MI DMII Medical ManagementDocument52 pagesAcute MI DMII Medical ManagementsherwincruzNo ratings yet
- Nuggets Combined - Indexed + Searchable PDFDocument478 pagesNuggets Combined - Indexed + Searchable PDFjasleenNo ratings yet
- Nursing Care of HydronephrosisDocument19 pagesNursing Care of Hydronephrosisvictor zhefaNo ratings yet
- MD3150E Epidemiology, Biostatistics and Public Health Week 6Document30 pagesMD3150E Epidemiology, Biostatistics and Public Health Week 6Juma AwarNo ratings yet
- Portal HypertensionDocument25 pagesPortal HypertensionJainab SiddiquiNo ratings yet
- Arthritis E-Book DF PDFDocument14 pagesArthritis E-Book DF PDFManuel Anthony Lopez0% (1)
- Toxic Responses of The Endocrine SystemDocument38 pagesToxic Responses of The Endocrine SystemPingNo ratings yet
- Oxygen DeliveryDocument6 pagesOxygen Deliveryyourdirtysocks100% (1)
- MCN Quiz 2Document6 pagesMCN Quiz 2Romer RiveraNo ratings yet
- Medical-Surgical Nursing 1Document28 pagesMedical-Surgical Nursing 1Maui Ting100% (1)