You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Principles of Transactional Analysis - by Eric BerneDocument8 pagesPrinciples of Transactional Analysis - by Eric BernecornelpcNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Gait Analysis: Prerequisite of Normal GaitDocument4 pagesGait Analysis: Prerequisite of Normal GaitKieran Levi100% (1)
- Packrat Cardio QuestionsDocument63 pagesPackrat Cardio Questionscrystalshe100% (1)
- Hospital Job DescriptionsDocument48 pagesHospital Job DescriptionsLoresita Amoranto Rebong RNNo ratings yet
- Emotional Causes of CancerDocument6 pagesEmotional Causes of CancerstudiocrocNo ratings yet
- Circulatory SystemDocument21 pagesCirculatory SystemKumar Sujeet100% (1)
- AnupanaDocument60 pagesAnupanaVaidya Nur50% (4)
- Thyroid Gland AnatomyDocument11 pagesThyroid Gland AnatomyRem AlfelorNo ratings yet
- Pink Panther - Diabetes Management - Chapter 9Document16 pagesPink Panther - Diabetes Management - Chapter 9jennmoyerNo ratings yet
- Dressing and BandagingDocument5 pagesDressing and BandagingMaricar Gallamora Dela CruzNo ratings yet
- Master Tong-Style Acupuncturist Interview Part 1Document4 pagesMaster Tong-Style Acupuncturist Interview Part 1Anonymous uMnup2r100% (1)
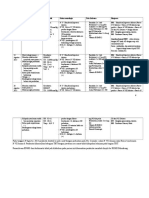
- Follow Up: Tanggal Keluhan Tanda Vital Status Neurologis Tata Laksana Diagnosa DKDocument2 pagesFollow Up: Tanggal Keluhan Tanda Vital Status Neurologis Tata Laksana Diagnosa DKSparkling PinkNo ratings yet
- TTIKDocument50 pagesTTIKSparkling PinkNo ratings yet
- Dyslexia (From Yale)Document4 pagesDyslexia (From Yale)Sparkling PinkNo ratings yet
- 5.daftar Pustaka Ramsay Hunt SyndromeDocument3 pages5.daftar Pustaka Ramsay Hunt SyndromeSparkling PinkNo ratings yet
- Myelopathy (Spine)Document34 pagesMyelopathy (Spine)Sparkling PinkNo ratings yet
- Penda Hulu AnDocument4 pagesPenda Hulu AnSparkling PinkNo ratings yet
- Perdarahan SubaraknoidDocument7 pagesPerdarahan SubaraknoidJessica SilaenNo ratings yet
- Bruits of The Head and Neck (Wildchild)Document6 pagesBruits of The Head and Neck (Wildchild)Sparkling PinkNo ratings yet
- Hipertrigliseridemia in PregnancyDocument5 pagesHipertrigliseridemia in PregnancySparkling PinkNo ratings yet
- ALS Amyotrophic Lateral Sclerosis Literature Review 1 - 14Document11 pagesALS Amyotrophic Lateral Sclerosis Literature Review 1 - 14Sparkling PinkNo ratings yet
- Jadwal Jaga Residen April 2016Document2 pagesJadwal Jaga Residen April 2016Sparkling PinkNo ratings yet
- Diabetes Mellitus in PregnancyDocument12 pagesDiabetes Mellitus in PregnancyFadila R. Lubis LubisNo ratings yet
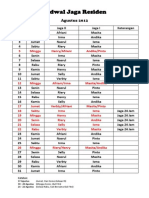
- On Call Schedule, Night Shift Schedule, Hospital, Residency Program, Neurology, Life, August 2012. Tentative Program.Document2 pagesOn Call Schedule, Night Shift Schedule, Hospital, Residency Program, Neurology, Life, August 2012. Tentative Program.Sparkling PinkNo ratings yet
- Daftar Pustaka ALSDocument2 pagesDaftar Pustaka ALSSparkling PinkNo ratings yet
- On-Call Schedule: August 2012Document2 pagesOn-Call Schedule: August 2012Sparkling PinkNo ratings yet
- Effects of Vitamin E On Stroke SubtypesDocument17 pagesEffects of Vitamin E On Stroke SubtypesSparkling PinkNo ratings yet
- Orthovoltage Vs MegavoltageDocument7 pagesOrthovoltage Vs MegavoltageEmmanuel Cuevas MisNo ratings yet
- Buklet Amt 01 EnglishDocument13 pagesBuklet Amt 01 Englishaemrana100% (1)
- RBC and WBC Identification Under MicroscopeDocument7 pagesRBC and WBC Identification Under MicroscopeHriday jyoti DekaNo ratings yet
- Resp 1.02 Hierarchy of O2 Delivery MethodsDocument1 pageResp 1.02 Hierarchy of O2 Delivery MethodsVin Lorenzo CampbellNo ratings yet
- Not Eligible As No Experience of Teaching and ResearchDocument5 pagesNot Eligible As No Experience of Teaching and ResearchVasanth Kumar AllaNo ratings yet
- Teen Pregnancy Rates in BoliviaDocument2 pagesTeen Pregnancy Rates in BoliviaVanessa Sandoval Aguilera100% (1)
- Combat Lifesaver Guide to One-Person Bag Valve Mask VentilationDocument1 pageCombat Lifesaver Guide to One-Person Bag Valve Mask VentilationSae TumNo ratings yet
- Detyre Kursi: Lenda:AnglishtDocument11 pagesDetyre Kursi: Lenda:AnglishtFjorelo FeroNo ratings yet
- Comparing MUAC and weight-for-height to diagnose SAMDocument30 pagesComparing MUAC and weight-for-height to diagnose SAMsidhant pundhirNo ratings yet
- New 5Document37 pagesNew 5rishi gupta100% (1)
- Mayo HospitalDocument1 pageMayo HospitalTooba SaeedNo ratings yet
- Aj. Chulaporn-Bosutinib-Search Engine and Study EndpointsDocument5 pagesAj. Chulaporn-Bosutinib-Search Engine and Study EndpointsCalm Phurit SenachaiNo ratings yet
- 13497-Texto Del Artículo-48998-1-10-20150925Document7 pages13497-Texto Del Artículo-48998-1-10-20150925Pipe Contecha BernatteNo ratings yet
- Diet CounsellingDocument11 pagesDiet CounsellingDrBhawna AroraNo ratings yet
- 53 Vol. 6 Issue 7 IJPSR 2015 RA 4953Document9 pages53 Vol. 6 Issue 7 IJPSR 2015 RA 4953Dina AyupnNo ratings yet
- BHP Formula No 55 Refrence - Bioplasgen 20 Homeopathic Medicine For Skin DiseasesDocument2 pagesBHP Formula No 55 Refrence - Bioplasgen 20 Homeopathic Medicine For Skin DiseasesKazy Habibur RahmanNo ratings yet
- Register Now for the 3rd Hematology Forum 2023Document1 pageRegister Now for the 3rd Hematology Forum 2023modather sanosiNo ratings yet
- Types of Casts and Their IndicationsDocument3 pagesTypes of Casts and Their IndicationsPhylum ChordataNo ratings yet
- Punjab Healthcare Commission: CG-09RM-Ed2Document168 pagesPunjab Healthcare Commission: CG-09RM-Ed2saimaNo ratings yet