You might also like
- Art 2Document6 pagesArt 2Joyce Stefania Posada MauricioNo ratings yet
- How to effectively use a 264 applianceDocument11 pagesHow to effectively use a 264 appliancevefiisphepy83312No ratings yet
- Clear Aligner: Invisalign: A ReviewDocument3 pagesClear Aligner: Invisalign: A ReviewHARITHA H.PNo ratings yet
- 8907 1yk4o27Document6 pages8907 1yk4o27Zahid ManzoorNo ratings yet
- PII0022391383903438Document5 pagesPII0022391383903438Vivek LathNo ratings yet
- Cleft Lip and Palate: MethodologyDocument25 pagesCleft Lip and Palate: MethodologyTahani AlmagrhiNo ratings yet
- Eroglu2019 PDFDocument7 pagesEroglu2019 PDFHamza GaaloulNo ratings yet
- Dentoalveolar Effects of Removable vs Fixed Cribs in Open Bite TreatmentDocument7 pagesDentoalveolar Effects of Removable vs Fixed Cribs in Open Bite TreatmentTesisTraduccionesRuzelNo ratings yet
- Stability of Class II Malocclusion Treatment With The Distal Jet Followed by Fixed AppliancesDocument8 pagesStability of Class II Malocclusion Treatment With The Distal Jet Followed by Fixed AppliancesFabian BarretoNo ratings yet
- Gingival Margin Stability After Mucogingival Plastic Surgery. The Effect of Manual Versus Powered Toothbrushing: A Randomized Clinical TrialDocument13 pagesGingival Margin Stability After Mucogingival Plastic Surgery. The Effect of Manual Versus Powered Toothbrushing: A Randomized Clinical TrialMarco Antonio García LunaNo ratings yet
- JR OrthoDocument23 pagesJR OrthoDwi Putro SetiyantomoNo ratings yet
- Review Article: Karoon AgrawalDocument9 pagesReview Article: Karoon Agrawalshagun singhNo ratings yet
- How To Effectively Use A 264 Appliance: Features SectionDocument11 pagesHow To Effectively Use A 264 Appliance: Features SectionJulio Ugás ZapataNo ratings yet
- Lingual Orthodontics - A Review: Invited ArticlesDocument8 pagesLingual Orthodontics - A Review: Invited ArticlesVerghese George MNo ratings yet
- Management of Posterior Ankyloglossia and Upper Lip Ties in A Tertiary Otolaryngology Outpatient ClinicDocument4 pagesManagement of Posterior Ankyloglossia and Upper Lip Ties in A Tertiary Otolaryngology Outpatient Clinicadrian bouzasNo ratings yet
- Removable Orthodontic Appliances: New Perspectives On Capabilities and EfficiencyDocument6 pagesRemovable Orthodontic Appliances: New Perspectives On Capabilities and EfficiencyYosu Obok HermanlieNo ratings yet
- Combination Syndrome Bone Loss PreventionDocument9 pagesCombination Syndrome Bone Loss PreventionAmar BimavarapuNo ratings yet
- Thesis Copy 6 CorrectedDocument54 pagesThesis Copy 6 CorrectedanushiNo ratings yet
- CCR3 8 1932Document5 pagesCCR3 8 1932Alice EmailsNo ratings yet
- Developing An Instrument To Support Oral Care in The ElderlyDocument6 pagesDeveloping An Instrument To Support Oral Care in The ElderlyGermán PuigNo ratings yet
- Immediate Versus Conventional Loading For The Maxilla With Implants Placed Into Fresh and Healed Extraction Sites To Support A Full-Arch Fixed Prosthesis - Nonrandomized Controlled Clinical StudyDocument9 pagesImmediate Versus Conventional Loading For The Maxilla With Implants Placed Into Fresh and Healed Extraction Sites To Support A Full-Arch Fixed Prosthesis - Nonrandomized Controlled Clinical StudySTEPHANIE JARAMILLONo ratings yet
- Open Bite Retention ProtocolDocument13 pagesOpen Bite Retention ProtocolChirag PatilNo ratings yet
- Management of Vertical Maxillary ExcessDocument24 pagesManagement of Vertical Maxillary ExcesssweetieNo ratings yet
- A Unique Habit-Breaking Therapy: An Innovative Approach (PKS Approach)Document3 pagesA Unique Habit-Breaking Therapy: An Innovative Approach (PKS Approach)IJAR JOURNALNo ratings yet
- MGMT FrenulumDocument13 pagesMGMT FrenulumEkta KhobragadeNo ratings yet
- Cleft Treatment Obturpaedics Orthopaeddontics Orthodontics Important ConceptsDocument5 pagesCleft Treatment Obturpaedics Orthopaeddontics Orthodontics Important ConceptsAthenaeum Scientific PublishersNo ratings yet
- Orthodontic Open BiteDocument29 pagesOrthodontic Open BiteAbboodNo ratings yet
- Orthodontics: Myofunctional AppliancesDocument10 pagesOrthodontics: Myofunctional AppliancesSaif HashimNo ratings yet
- C01251115Document5 pagesC01251115agnes herlinaNo ratings yet
- Analysis of Masticatory Cycle EfficiencyDocument4 pagesAnalysis of Masticatory Cycle EfficiencyAndreeaSinNo ratings yet
- Mandibular Incisor Alignment in Untreated Subjects Compared With Long-Term Changes After OrthodonticDocument9 pagesMandibular Incisor Alignment in Untreated Subjects Compared With Long-Term Changes After OrthodonticPAOLA IVETTE MARTINEZ RODRIGUEZNo ratings yet
- Effect of Denture Cleansing Solutions On The Retention of Locator Attachments Over Time.Document18 pagesEffect of Denture Cleansing Solutions On The Retention of Locator Attachments Over Time.Nubia amparo Poveda GonzálezNo ratings yet
- Case ReportDocument3 pagesCase ReportZahra HayunaNo ratings yet
- Tnmgrmu DissertationDocument4 pagesTnmgrmu DissertationHelpWithAPaperNewOrleans100% (1)
- EJMCM - Volume 7 - Issue 4 - Pages 1689-1693Document5 pagesEJMCM - Volume 7 - Issue 4 - Pages 1689-1693Tanushree JainNo ratings yet
- The Retention Characteristics of Hawley and Vacuum-FormedDocument8 pagesThe Retention Characteristics of Hawley and Vacuum-FormedYayis LondoñoNo ratings yet
- The Hall Technique: Food for ThoughtDocument50 pagesThe Hall Technique: Food for ThoughtMustafa Tambawala100% (1)
- Another Tie After Tongue Tie SurgeryDocument4 pagesAnother Tie After Tongue Tie SurgeryPaulina SandovalNo ratings yet
- Pain Control and Carious Primary TeethDocument3 pagesPain Control and Carious Primary TeethmirfanulhaqNo ratings yet
- Modified Oral Screen Case ReportDocument9 pagesModified Oral Screen Case Reportfayasyabmin100% (1)
- Rapid Palatal ExpanderDocument28 pagesRapid Palatal ExpandertonhanrhmNo ratings yet
- Twin Blok 4Document11 pagesTwin Blok 4KosanKucingGendutPurwokertoNo ratings yet
- Short-And Long-Term Evaluation of Mandibular Dental Arch Dimensional Changes in Patients Treated With A Lip Bumper During Mixed Dentition Followed by Fixed AppliancesDocument8 pagesShort-And Long-Term Evaluation of Mandibular Dental Arch Dimensional Changes in Patients Treated With A Lip Bumper During Mixed Dentition Followed by Fixed AppliancesGABRIELA NIETO GONZALEZNo ratings yet
- Open-Cap Acrylic SplintDocument3 pagesOpen-Cap Acrylic SplintFeras Al-ZbounNo ratings yet
- Occlusal Contacts RetentionDocument9 pagesOcclusal Contacts RetentionRockey ShrivastavaNo ratings yet
- Modified Palatal Crib Appliance For Habit Correction: A Case ReportDocument5 pagesModified Palatal Crib Appliance For Habit Correction: A Case ReportPutri Tasya ANo ratings yet
- Impact of Removable Partial Denture Prosthesis On Chewing EfficiencyDocument5 pagesImpact of Removable Partial Denture Prosthesis On Chewing EfficiencyMădălina ConstantinNo ratings yet
- The Complete Denture Prosthesis: Clinical and Laboratory Applications - Insertion, Patient Adaptation, and Post-Insertion CareDocument16 pagesThe Complete Denture Prosthesis: Clinical and Laboratory Applications - Insertion, Patient Adaptation, and Post-Insertion CareAnimeAngelNo ratings yet
- Esthetic Orthodontic TreatmentDocument20 pagesEsthetic Orthodontic TreatmenteutaNo ratings yet
- Testori - Workshop Guidlines On Immediate Loading in Implant DentistryDocument6 pagesTestori - Workshop Guidlines On Immediate Loading in Implant DentistryÄpriolia SuNo ratings yet
- Fixed Versus Removable Orthodontic Appliances To Correct Anterior Crossbite in The Mixed Dentition-A Randomized Controlled Trial PDFDocument6 pagesFixed Versus Removable Orthodontic Appliances To Correct Anterior Crossbite in The Mixed Dentition-A Randomized Controlled Trial PDFJejeNo ratings yet
- Palatally Impacted CaninesDocument5 pagesPalatally Impacted CaninesMoisés MartinsNo ratings yet
- 30SuctiondenturesVOL4ISSUE4PP108-111 20181017082305Document4 pages30SuctiondenturesVOL4ISSUE4PP108-111 20181017082305Mutia SariayuNo ratings yet
- Treatment Approach: Complete Cleft Lip and PalateDocument20 pagesTreatment Approach: Complete Cleft Lip and PalateTengku Risyana RumansyahNo ratings yet
- Policy On Management of The Frenulum inDocument6 pagesPolicy On Management of The Frenulum inمعتزباللهNo ratings yet
- Jurnal ObturatorDocument4 pagesJurnal ObturatorEuginia YosephineNo ratings yet
- Effect of Desensitizing Patch For Dentin Hypersensitivity: Su-Yeon Park, Mi-Ra Lee, Jin-Hee WonDocument7 pagesEffect of Desensitizing Patch For Dentin Hypersensitivity: Su-Yeon Park, Mi-Ra Lee, Jin-Hee WonIndah LestariNo ratings yet
- Open Drainage or NotDocument6 pagesOpen Drainage or Notjesuscomingsoon2005_No ratings yet
- 10 1067@mpr 2000 107113Document7 pages10 1067@mpr 2000 107113gbaez.88No ratings yet
- Minimally Invasive Approaches in Endodontic PracticeFrom EverandMinimally Invasive Approaches in Endodontic PracticeGianluca PlotinoNo ratings yet
- Full Veneer Versus Traditional Veneer Preparation - A Discussion of Interproximal ExtensionDocument5 pagesFull Veneer Versus Traditional Veneer Preparation - A Discussion of Interproximal ExtensionDr. Zardasht N. BradostyNo ratings yet
- Proyecto Final Ángela P. FierroDocument39 pagesProyecto Final Ángela P. Fierro9bh4spchgsNo ratings yet
- Dance and Health: Christina Pham Mr. Schurtz AP English 12: Period 4/5 5/17/11Document58 pagesDance and Health: Christina Pham Mr. Schurtz AP English 12: Period 4/5 5/17/11cpham8792No ratings yet
- Case Report Enlargement GinggivaDocument3 pagesCase Report Enlargement GinggivaAnindya LaksmiNo ratings yet
- Prefinal ProgramDocument1 pagePrefinal ProgramHussein AhmedNo ratings yet
- DHA A1 - Corrected DHA QuestionsDocument21 pagesDHA A1 - Corrected DHA QuestionsFarha Navas100% (1)
- Pre Prosthetic Surgery PDFDocument107 pagesPre Prosthetic Surgery PDFdrkavintNo ratings yet
- Eyeguide 1Document23 pagesEyeguide 1Ammor AdnaneNo ratings yet
- English For Dentistry 2021Document30 pagesEnglish For Dentistry 2021Seyna Official100% (2)
- Class 5 & Above Project Detailing-1Document4 pagesClass 5 & Above Project Detailing-1ik62299No ratings yet
- Buku Menu - Regio - 1. Diy-Jateng 2Document11 pagesBuku Menu - Regio - 1. Diy-Jateng 2PARK TATACHIMCHIMNo ratings yet
- N N T I R: Asogastric and Asoenteric Ube Nsertion and EmovalDocument8 pagesN N T I R: Asogastric and Asoenteric Ube Nsertion and EmovalFernanda AlfaroNo ratings yet
- Anexo 3 DESCRIBING APPEARANCEDocument4 pagesAnexo 3 DESCRIBING APPEARANCELucia A Gomez MNo ratings yet
- 2 Internal Anatomy of TeethDocument113 pages2 Internal Anatomy of TeethAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Chapter 5 (Fundamentals of Cavity Preparation) Choose The Most Suitable AnswerDocument13 pagesChapter 5 (Fundamentals of Cavity Preparation) Choose The Most Suitable AnswerAbo QadeerNo ratings yet
- Investrigatory Project (Term I) : Subject - BIOLOGYDocument20 pagesInvestrigatory Project (Term I) : Subject - BIOLOGYRehan RazaNo ratings yet
- Dental Anatomy - WEEK 1 Basic Terminology For Understanding Tooth Morphology Quiz 1, Chapter 1Document8 pagesDental Anatomy - WEEK 1 Basic Terminology For Understanding Tooth Morphology Quiz 1, Chapter 1GlassyNo ratings yet
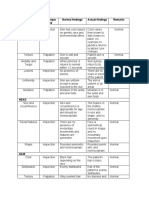
- Area Assessed Technique Used Normal Findings Actual Findings Remarks SkinDocument6 pagesArea Assessed Technique Used Normal Findings Actual Findings Remarks SkinLadybelle GototosNo ratings yet
- Early Otorrhea RatesDocument26 pagesEarly Otorrhea RatesRhea Andrea UyNo ratings yet
- Cleft Lip & PalateDocument13 pagesCleft Lip & PalateMahsaNo ratings yet
- Benign Lesions of LarynxDocument1 pageBenign Lesions of LarynxAnjana UNo ratings yet
- BF Periapical Lucency NEL ARI VENDocument22 pagesBF Periapical Lucency NEL ARI VENdiniNo ratings yet
- Hair and Nail DisordersDocument42 pagesHair and Nail DisordersSantosh ThapaNo ratings yet
- Case History EndodonticsDocument1 pageCase History EndodonticsDurva JainNo ratings yet
- UntitledDocument5 pagesUntitledCelsa AndreanNo ratings yet
- Zygomatic Implants for the Extramaxillary ApproachDocument24 pagesZygomatic Implants for the Extramaxillary ApproachLê Minh KhôiNo ratings yet
- 4 - History, Physical Examination, and The Preoperative EvaluationDocument17 pages4 - History, Physical Examination, and The Preoperative EvaluationMauricio Ruiz MoralesNo ratings yet
- General Guidelines For Skin CareDocument4 pagesGeneral Guidelines For Skin CareDaesungNo ratings yet
- Management of A Large Cyst in Maxillary Region: A Case ReportDocument11 pagesManagement of A Large Cyst in Maxillary Region: A Case ReportAry NohuNo ratings yet
- 23 External Ear (Done)Document4 pages23 External Ear (Done)osamaeNo ratings yet