You might also like
- How To: Read ECG?Document63 pagesHow To: Read ECG?Let BNo ratings yet
- Arrythmias and EKGs 2Document20 pagesArrythmias and EKGs 2Nur Ima ErvianaNo ratings yet
- Avnrt AvrtDocument21 pagesAvnrt AvrtRima Rovanne Wenas100% (1)
- EKG Taki-Bradi AritmiaDocument47 pagesEKG Taki-Bradi Aritmiamithaa octoviagnesNo ratings yet
- Introduction To ECG RhythmsDocument59 pagesIntroduction To ECG RhythmsIvona RagužNo ratings yet
- ECG InterpretationDocument41 pagesECG InterpretationgjdbfiuvaNo ratings yet
- Arrhythmias GeneralDocument131 pagesArrhythmias GeneralAnonymous IRl5fn6No ratings yet
- Approach To ArrhythmiasDocument1 pageApproach To ArrhythmiasADITYA SARANGINo ratings yet
- Approach To ACLS RhythmDocument150 pagesApproach To ACLS RhythmChristine Bernadette Rapal Bollong100% (2)
- Tachycardia Which Fast Is Too FuriousDocument79 pagesTachycardia Which Fast Is Too FuriousEstiningtiyas RahayuNo ratings yet
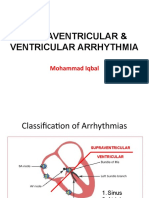
- Supraventrikular & Ventrikular ArrhytmiaDocument65 pagesSupraventrikular & Ventrikular ArrhytmiarosyadNo ratings yet
- PG - Quick Look On Arrhythmia in ED - JCU 2021Document71 pagesPG - Quick Look On Arrhythmia in ED - JCU 2021Afied FitrahNo ratings yet
- Muzakkir-Takikardi PDFDocument32 pagesMuzakkir-Takikardi PDFThono HartonoNo ratings yet
- CardiologyDocument149 pagesCardiologyMuhammad SyafiqNo ratings yet
- Ecg enDocument12 pagesEcg enKeep smileNo ratings yet
- Intern TutorialDocument288 pagesIntern TutorialtoffeepolNo ratings yet
- ECG ReviewDocument146 pagesECG ReviewThea DinoNo ratings yet
- Ecg Criteria SVT Vs VT: DR - Vinoth Kumar PostgraduateDocument48 pagesEcg Criteria SVT Vs VT: DR - Vinoth Kumar Postgraduatelichumo murryNo ratings yet
- SVT CaseDocument11 pagesSVT CaseZakiy AzzuhdiNo ratings yet
- Rhythm Description Schematic Diagram Egc Characteristics Sample TraceDocument6 pagesRhythm Description Schematic Diagram Egc Characteristics Sample TraceJhenne Kyle Ko Dee100% (1)
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- Curs 7 - Bradiaritmii TahiaritmiiDocument88 pagesCurs 7 - Bradiaritmii Tahiaritmiijhonny12321No ratings yet
- Atrial-Rhythm 230518 191520-1Document2 pagesAtrial-Rhythm 230518 191520-1Maxinne GorospeNo ratings yet
- Understanding ECG's 2Document41 pagesUnderstanding ECG's 2Ben HarperNo ratings yet
- ArrhytmiaDocument70 pagesArrhytmiaAfied FitrahNo ratings yet
- ECG Arrhythmia2006Document28 pagesECG Arrhythmia2006rickyfauzanNo ratings yet
- ECG Arrhythmia2006Document28 pagesECG Arrhythmia2006aris rifkhiNo ratings yet
- Basic ArrythmiasDocument58 pagesBasic ArrythmiasZachary Cohen100% (1)
- Supraventricular Arrhythmias: Dr. Arun Srinivas Chief Cardiologist Vikram Hospital, MysoreDocument81 pagesSupraventricular Arrhythmias: Dr. Arun Srinivas Chief Cardiologist Vikram Hospital, Mysorerobinjohn06No ratings yet
- Supraventricular TachyarrythmiasDocument24 pagesSupraventricular TachyarrythmiasEINSTEIN2DNo ratings yet
- Kuliah Ekg UnswagatiDocument75 pagesKuliah Ekg UnswagatiiikNo ratings yet
- ECG ArrhythmiaDocument27 pagesECG ArrhythmiaSrikitta DanieliaNo ratings yet
- W-2-Sevigny-Basic ECG PDFDocument61 pagesW-2-Sevigny-Basic ECG PDFdheaNo ratings yet
- Nclex RN Review Notes 2018 Triple eDocument30 pagesNclex RN Review Notes 2018 Triple eEndla SriniNo ratings yet
- ECG Reading: The Common and DangerousDocument77 pagesECG Reading: The Common and DangerousFitri UlansariNo ratings yet
- Supraventricular Tachycardia - Life in The Fast Lane ECG LibraryDocument29 pagesSupraventricular Tachycardia - Life in The Fast Lane ECG LibraryYehuda Agus SantosoNo ratings yet
- Sunday Academic MeetDocument22 pagesSunday Academic MeetSrinivasan YashrajNo ratings yet
- All EcgDocument143 pagesAll EcgYenza FaheraNo ratings yet
- Ecg Pathology 02Document95 pagesEcg Pathology 02Andi MP Manurung100% (1)
- KULIAH ECG Dinkes PurworejoDocument69 pagesKULIAH ECG Dinkes PurworejoVella NurfatimahNo ratings yet
- Cardiac Arrhythmia 171209212142 2Document74 pagesCardiac Arrhythmia 171209212142 2Gunel Sadiqova100% (1)
- Aina ArrhytmiaDocument2 pagesAina ArrhytmiaNur Fatima SanaaniNo ratings yet
- Atria Arrythmia TestDocument8 pagesAtria Arrythmia TestAnnette SandovalNo ratings yet
- Aritmia - DR IqbalDocument49 pagesAritmia - DR IqbalANISA SALAMAHNo ratings yet
- Kuliah EKG II Unswagati 2016Document77 pagesKuliah EKG II Unswagati 2016iikNo ratings yet
- Width of The QRS Complex: - Wide VT, SVT With Aberrant Conduction - Narrrow SVTDocument11 pagesWidth of The QRS Complex: - Wide VT, SVT With Aberrant Conduction - Narrrow SVTWidelmark FarrelNo ratings yet
- ELECTROCARDIOGRAPHYDocument75 pagesELECTROCARDIOGRAPHYMeliaNo ratings yet
- Beta's Short RP.: Click Here To ViewDocument1 pageBeta's Short RP.: Click Here To ViewLwin Maung Maung ThikeNo ratings yet
- Cardiac Life Support Cme Latest Edited VersionDocument53 pagesCardiac Life Support Cme Latest Edited VersionSyed Shahrul Naz SyedNo ratings yet
- Cardiac Life Support Cme Latest Edited VersionDocument53 pagesCardiac Life Support Cme Latest Edited VersionSyed Shahrul Naz SyedNo ratings yet
- KULIAH ECG Dinkes PurworejoDocument69 pagesKULIAH ECG Dinkes PurworejoSofian PalupiNo ratings yet
- Cheat ECGDocument3 pagesCheat ECGNeil Emman BotardoNo ratings yet
- Ecg Interpretation:: The BasicsDocument40 pagesEcg Interpretation:: The BasicsRavi SharmaNo ratings yet
- s1c11 ECG - Supplement PDFDocument108 pagess1c11 ECG - Supplement PDFVisan Andreea Mihaela RamonaNo ratings yet
- Ekg LetalDocument50 pagesEkg LetalKusmawan IdNo ratings yet
- The ECG Made Easy by John R. HamptonDocument1 pageThe ECG Made Easy by John R. HamptonLpNo ratings yet
- Learning ECGDocument187 pagesLearning ECGPhysiology by Dr Raghuveer100% (2)
- 22 Disritmia 2018Document60 pages22 Disritmia 2018Nur akilaNo ratings yet
- Useful Methods in CatiaDocument30 pagesUseful Methods in CatiaNastase Corina100% (2)
- Gifted Black Females Attending Predominantly White Schools Compressed 1 CompressedDocument488 pagesGifted Black Females Attending Predominantly White Schools Compressed 1 Compressedapi-718408484No ratings yet
- Chemical Classification of HormonesDocument65 pagesChemical Classification of HormonesetNo ratings yet
- Book Review Fiction New HereDocument7 pagesBook Review Fiction New HereFILZAH SYAUQINA BINTI SUBLY Pelajar KPTM IpohNo ratings yet
- Line Integrals in The Plane: 4. 4A. Plane Vector FieldsDocument7 pagesLine Integrals in The Plane: 4. 4A. Plane Vector FieldsShaip DautiNo ratings yet
- Malampaya Case StudyDocument15 pagesMalampaya Case StudyMark Kenneth ValerioNo ratings yet
- Financial Statement AnalysisDocument18 pagesFinancial Statement AnalysisAbdul MajeedNo ratings yet
- Case StudyDocument2 pagesCase StudyFadhlin Sakina SaadNo ratings yet
- Case Study Analysis - WeWorkDocument8 pagesCase Study Analysis - WeWorkHervé Kubwimana50% (2)
- Eco EssayDocument3 pagesEco EssaymanthanNo ratings yet
- I. Objectives:: Semi-Detailed Lesson Plan in Reading and Writing (Grade 11)Document5 pagesI. Objectives:: Semi-Detailed Lesson Plan in Reading and Writing (Grade 11)Shelton Lyndon CemanesNo ratings yet
- Conjunctions in SentencesDocument8 pagesConjunctions in SentencesPunitha PoppyNo ratings yet
- Retail Visibility Project of AircelDocument89 pagesRetail Visibility Project of Aircelabhishekkraj100% (1)
- Ultrasonic Based Distance Measurement SystemDocument18 pagesUltrasonic Based Distance Measurement SystemAman100% (2)
- The Consulting Industry and Its Transformations in WordDocument23 pagesThe Consulting Industry and Its Transformations in Wordlei ann magnayeNo ratings yet
- Bakteri Anaerob: Morfologi, Fisiologi, Epidemiologi, Diagnosis, Pemeriksaan Sy. Miftahul El J.TDocument46 pagesBakteri Anaerob: Morfologi, Fisiologi, Epidemiologi, Diagnosis, Pemeriksaan Sy. Miftahul El J.TAlif NakyukoNo ratings yet
- So Tim Penilik N10 16 Desember 2022 Finish-1Document163 pagesSo Tim Penilik N10 16 Desember 2022 Finish-1Muhammad EkiNo ratings yet
- Session 1: Strategic Marketing - Introduction & ScopeDocument38 pagesSession 1: Strategic Marketing - Introduction & ScopeImrul Hasan ChowdhuryNo ratings yet
- Beer Lambert'S Law: Dr. Swastika Das Professor of ChemistryDocument19 pagesBeer Lambert'S Law: Dr. Swastika Das Professor of ChemistryShabanaNo ratings yet
- Introduction To Pharmacology by ZebDocument31 pagesIntroduction To Pharmacology by ZebSanam MalikNo ratings yet
- DU Series MCCB CatalogueDocument8 pagesDU Series MCCB Cataloguerobinknit2009No ratings yet
- Saes T 883Document13 pagesSaes T 883luke luckyNo ratings yet
- Facultybooklet2011-2012final - 006 (Unlocked by WWW - Freemypdf.com)Document199 pagesFacultybooklet2011-2012final - 006 (Unlocked by WWW - Freemypdf.com)kalam19892209No ratings yet
- Bai Tap Av 12 Thi Diem Unit TwoDocument7 pagesBai Tap Av 12 Thi Diem Unit TwonguyenngocquynhchiNo ratings yet
- Alem Ketema Proposal NewDocument25 pagesAlem Ketema Proposal NewLeulNo ratings yet
- 3 A Sanitary Standards Quick Reference GuideDocument98 pages3 A Sanitary Standards Quick Reference GuideLorettaMayNo ratings yet
- TOR AND SCOPING Presentation SlidesDocument23 pagesTOR AND SCOPING Presentation SlidesSRESTAA BHATTARAINo ratings yet
- Gummy Bear Story RubricDocument1 pageGummy Bear Story Rubricapi-365008921No ratings yet
- Basler Electric TCCDocument7 pagesBasler Electric TCCGalih Trisna NugrahaNo ratings yet
- Demand Determinants EEMDocument22 pagesDemand Determinants EEMPrabha KaranNo ratings yet