You might also like
- CC 8 Januari Gizi Buruk TSK HivDocument42 pagesCC 8 Januari Gizi Buruk TSK HivAisya FikritamaNo ratings yet
- CC 14 Mei 2017 Diare AkutDocument31 pagesCC 14 Mei 2017 Diare AkutDwi Pratika AnjarwatiNo ratings yet
- Lapkas Marasmus JadiDocument48 pagesLapkas Marasmus JadiRivhan FauzanNo ratings yet
- Case Conference DiareDocument47 pagesCase Conference DiareantogantengbangetzNo ratings yet
- Case Conference February 1st 2018Document26 pagesCase Conference February 1st 2018Efan StiawanNo ratings yet
- CC HCU Ped AnemiaDocument42 pagesCC HCU Ped AnemialatifahNo ratings yet
- Acute Nephrotic SyndromeDocument10 pagesAcute Nephrotic SyndromeEvi SilviaNo ratings yet
- DMDFDocument22 pagesDMDFsujal177402100% (1)
- CC 10 NOv 2017 ITPDocument32 pagesCC 10 NOv 2017 ITPLilik NatasubrataNo ratings yet
- Duty Report: Co-Assistant On Duty: Fadhila Ayu Safirina Succi Islami PDocument23 pagesDuty Report: Co-Assistant On Duty: Fadhila Ayu Safirina Succi Islami PDhila SafirinaNo ratings yet
- Case ReportDocument24 pagesCase ReportnuruldrNo ratings yet
- Morning Report Friday, Aug 11 2018Document51 pagesMorning Report Friday, Aug 11 2018Efan StiawanNo ratings yet
- Case MorbiliDocument49 pagesCase MorbiliSiLpi HamidiyahNo ratings yet
- Morning Report: Disusun Oleh: Devy Puspo WardoyoDocument36 pagesMorning Report: Disusun Oleh: Devy Puspo WardoyodevyNo ratings yet
- Case Conference Saturday Night Shift, APRIL 6 TH, 2019Document46 pagesCase Conference Saturday Night Shift, APRIL 6 TH, 2019delfiaNo ratings yet
- Case Conference 201017 (Acute Tonsillopharingitis)Document40 pagesCase Conference 201017 (Acute Tonsillopharingitis)febrydwiNo ratings yet
- SUPERVISOR: Dr. Johannes Saing, M.Ked (Ped), Sp.A (K) : Presented By: Saravana Selvi Sanmugam (110100426)Document46 pagesSUPERVISOR: Dr. Johannes Saing, M.Ked (Ped), Sp.A (K) : Presented By: Saravana Selvi Sanmugam (110100426)Saravana Selvi SanmugamNo ratings yet
- Case Report Ii.1 Identification Ii.3 Phisycal ExaminationDocument10 pagesCase Report Ii.1 Identification Ii.3 Phisycal ExaminationMasayu Mutiara UtiNo ratings yet
- Seminar 2 (Paeds)Document31 pagesSeminar 2 (Paeds)Jonathan YeohNo ratings yet
- Aboy1 Y.O With Bronchopneumonia, Iron Deficiency, Leukocytosis and Hepatomegaly Suspected Hematological MalignanciesDocument28 pagesAboy1 Y.O With Bronchopneumonia, Iron Deficiency, Leukocytosis and Hepatomegaly Suspected Hematological Malignanciesayu_gultom29No ratings yet
- Case Asma TikaDocument45 pagesCase Asma TikaMainur TikaNo ratings yet
- Morning Report Sunday, 4 MARCH 2018Document30 pagesMorning Report Sunday, 4 MARCH 2018Efan StiawanNo ratings yet
- AnasarcaDocument54 pagesAnasarcaSulaiman TahsinNo ratings yet
- Case Conference Sunday Night Shift, October 14 2018Document26 pagesCase Conference Sunday Night Shift, October 14 2018Hendra WardhanaNo ratings yet
- Case Presentation YayaDocument26 pagesCase Presentation Yayayusufharkian100% (1)
- CC 3 April 19 Anemia CombustioDocument35 pagesCC 3 April 19 Anemia CombustioAisya FikritamaNo ratings yet
- Naufal Tejo Case DMDocument38 pagesNaufal Tejo Case DMFatimahalhabsyiNo ratings yet
- Gastroenteritis in ChildrenDocument48 pagesGastroenteritis in ChildrenKelsingra FitzChivalry FarseerNo ratings yet
- Case GNApsDocument47 pagesCase GNApsAndhika Hadi WirawanNo ratings yet
- Morning Report: Thursday, September 21st 2017Document6 pagesMorning Report: Thursday, September 21st 2017Bima Ryanda PutraNo ratings yet
- Nephrotic SyndromeDocument66 pagesNephrotic SyndromeNicole ChanNo ratings yet
- CC 29 Sept 2018 Massa MediastinumDocument63 pagesCC 29 Sept 2018 Massa MediastinumHendra WardhanaNo ratings yet
- English Case JaundiceDocument38 pagesEnglish Case JaundiceCavin HandokoNo ratings yet
- Case Conference Thursday Night Shift, September 4 2018Document47 pagesCase Conference Thursday Night Shift, September 4 2018Aisya FikritamaNo ratings yet
- MR BP Dan AsphyxiaDocument29 pagesMR BP Dan AsphyxiaRizky FajriNo ratings yet
- Case Report DyspepsiaDocument32 pagesCase Report DyspepsiaAnnisa AstariNo ratings yet
- Gastroenteritis FinalDocument26 pagesGastroenteritis FinalPingky khingthongNo ratings yet
- Case Report GastroenteritisDocument36 pagesCase Report GastroenteritisDaisy DuckNo ratings yet
- Anamnesis: Autoanamnesis On March 22 ND 2017 Chief Complaint General Weekness 1 Day AgoDocument25 pagesAnamnesis: Autoanamnesis On March 22 ND 2017 Chief Complaint General Weekness 1 Day AgoTebeNo ratings yet
- Sirosis HepatisDocument29 pagesSirosis HepatisXaverius da CunhaNo ratings yet
- Anemia Case Ppt-2 Mansa GowdaDocument31 pagesAnemia Case Ppt-2 Mansa GowdaSyeda AliyaNo ratings yet
- Myelodisplastic SyndromeDocument29 pagesMyelodisplastic SyndromeTiara RahmawatiNo ratings yet
- Anemia by Harsha BJDocument23 pagesAnemia by Harsha BJnaveen kumar kushwahaNo ratings yet
- Sample Case Presentation - Occult BacteremiaDocument51 pagesSample Case Presentation - Occult BacteremiaPrecious Gutierrez BagazinNo ratings yet
- Morning Report: Disusun Oleh: Devy Puspo WardoyoDocument34 pagesMorning Report: Disusun Oleh: Devy Puspo WardoyodevyNo ratings yet
- Case MalariaDocument58 pagesCase MalariaHade Guntur SNo ratings yet
- Case Conference Pneumonia 17-08-19Document43 pagesCase Conference Pneumonia 17-08-19Primadiati Nickyta SariNo ratings yet
- Morning Report Acute DiarrheaDocument21 pagesMorning Report Acute DiarrheaElisabeth ElidaNo ratings yet
- Neli Pastinar, Penkes UE, RPGN, SLE, Duty HannaDocument19 pagesNeli Pastinar, Penkes UE, RPGN, SLE, Duty HannaHanna GustinNo ratings yet
- CC 17 Feb 2017 1st Epilepsy OkeDocument43 pagesCC 17 Feb 2017 1st Epilepsy OkeLucky Yoga -satria NatasukmaNo ratings yet
- Presentasi Kasus Dokter Arif Cynthia NataliaDocument26 pagesPresentasi Kasus Dokter Arif Cynthia NataliaIntan SorayaNo ratings yet
- Grand ReportsDocument60 pagesGrand ReportsfilchibuffNo ratings yet
- Morning Report: Disusun Oleh: Devy Puspo WardoyoDocument43 pagesMorning Report: Disusun Oleh: Devy Puspo WardoyodevyNo ratings yet
- Hydom Lutheran HospitalDocument41 pagesHydom Lutheran HospitalFesto HakiNo ratings yet
- Drug Eruption: Case PresentationDocument59 pagesDrug Eruption: Case PresentationAtika Mayasari PutriNo ratings yet
- MR Dr. FIRA 31 Jan 2019Document29 pagesMR Dr. FIRA 31 Jan 2019Rizky FajriNo ratings yet
- Morning Report: Disusun Oleh: Noermawati DewiDocument34 pagesMorning Report: Disusun Oleh: Noermawati DewidevyNo ratings yet
- Morep 15 July IPDDocument14 pagesMorep 15 July IPDnadziradickyNo ratings yet
- Summarized CPG and PFCDocument62 pagesSummarized CPG and PFCnc.angel.niceNo ratings yet
- Cardiac Troponin T Is Not Increased in PatientsDocument5 pagesCardiac Troponin T Is Not Increased in PatientsAnanda Putri ImsezNo ratings yet
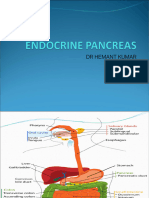
- Endocrine PancreasDocument21 pagesEndocrine Pancreaslacafey741No ratings yet
- ARGUMENTATIVE ESSAY - Windaa - 020Document4 pagesARGUMENTATIVE ESSAY - Windaa - 020winda oderaNo ratings yet
- Pacemakers - Fact SheetDocument7 pagesPacemakers - Fact Sheettalha.k.rajpootNo ratings yet
- Hepatology Research - 2023 - Yoshiji - Management of Cirrhotic Ascites Seven Step Treatment Protocol Based On The JapaneseDocument12 pagesHepatology Research - 2023 - Yoshiji - Management of Cirrhotic Ascites Seven Step Treatment Protocol Based On The JapaneseSarah FaziraNo ratings yet
- Covid 19 WorksheetsDocument16 pagesCovid 19 WorksheetsKarla Paola MoralesNo ratings yet
- SWAN Parkinson MRIDocument9 pagesSWAN Parkinson MRIulfi yunitaNo ratings yet
- The Effects of Laparoscopic Nissen FundoplicationDocument2 pagesThe Effects of Laparoscopic Nissen FundoplicationGabriel CassNo ratings yet
- Psychological Complication in PuerperiumDocument17 pagesPsychological Complication in Puerperiumbaby100% (2)
- 23-5-2022 Presentation JentadeutoDocument52 pages23-5-2022 Presentation JentadeutofsvtqsNo ratings yet
- The European Guideline On Management of Major Bleeding and Coagulopathy Following Trauma Sixth Edition (2023) PDFDocument1 pageThe European Guideline On Management of Major Bleeding and Coagulopathy Following Trauma Sixth Edition (2023) PDFMatheus LiraNo ratings yet
- Motor Neurone Disease: J GormallyDocument14 pagesMotor Neurone Disease: J GormallyBambang SutrisnoNo ratings yet
- Seizure Disorders: Assessment and Diagnostic FindingsDocument3 pagesSeizure Disorders: Assessment and Diagnostic FindingsBlessed GarcianoNo ratings yet
- BSS 2018Document24 pagesBSS 2018gumoha01No ratings yet
- Hypertensive CrisisDocument13 pagesHypertensive Crisis.Katherine CalderonNo ratings yet
- Ectopic Pregnancy Nursing Care PlansDocument27 pagesEctopic Pregnancy Nursing Care Plansviper7967880% (20)
- Operational Guidelines On FBMC With Sam PDFDocument84 pagesOperational Guidelines On FBMC With Sam PDFBalireddy NeeharikaNo ratings yet
- Contoh Soal Epilepsy and SeizureDocument4 pagesContoh Soal Epilepsy and SeizurejumasriNo ratings yet
- Case Study 1: Rhinitis AllergyDocument18 pagesCase Study 1: Rhinitis AllergyAsfiksia NeonatorumNo ratings yet
- Malabsorption SyndromeDocument7 pagesMalabsorption SyndromeHassan.shehri100% (4)
- Legal and Ethical Aspects of Genetic Screening and Counseling Role of Nurse in Genetic CounselingDocument41 pagesLegal and Ethical Aspects of Genetic Screening and Counseling Role of Nurse in Genetic CounselingAmy Lalringhluani67% (3)
- Safe Working EnvironmentDocument16 pagesSafe Working EnvironmentDawud AsnakewNo ratings yet
- Abdul Malik Hassim Lecturer DMA Management & Science UniversityDocument21 pagesAbdul Malik Hassim Lecturer DMA Management & Science UniversitykimmgizelleNo ratings yet
- 3M Bair Hugger Gown SystemDocument4 pages3M Bair Hugger Gown SystemmochkurniawanNo ratings yet
- Ebook John Murtaghs General Practice Companion Handbook PDF Full Chapter PDFDocument67 pagesEbook John Murtaghs General Practice Companion Handbook PDF Full Chapter PDFroberto.duncan209100% (27)
- ICU One Pager NIPPVDocument1 pageICU One Pager NIPPVNicholas HelmstetterNo ratings yet
- Re-Test SUBJECT-English Core Class - Xi Time: 2 Hrs. M.M: 50 General InstructionsDocument8 pagesRe-Test SUBJECT-English Core Class - Xi Time: 2 Hrs. M.M: 50 General InstructionsSunilDwivediNo ratings yet
- Health Grade10 4th QuarterDocument40 pagesHealth Grade10 4th QuarterYnjel HilarioNo ratings yet
- 2 Bachelor of Optometry (B Optom) 1Document7 pages2 Bachelor of Optometry (B Optom) 1Rehana ThapaNo ratings yet
- Acute Rheumatic FeverDocument39 pagesAcute Rheumatic FeverUzma BanoNo ratings yet