You might also like
- CS45385 NHS Abdo Pain Pathway Management - Primary Care Nov 17Document2 pagesCS45385 NHS Abdo Pain Pathway Management - Primary Care Nov 17Dinno PradanaNo ratings yet
- Fluid Managementuntuk Mahasiswa SajaDocument56 pagesFluid Managementuntuk Mahasiswa SajaPratami Rieuwpassa IINo ratings yet
- Assessing Seriously Ill PatientsDocument20 pagesAssessing Seriously Ill PatientsSianipar Mangara Wahyu CharrosNo ratings yet
- Headache Management in Primary CareDocument59 pagesHeadache Management in Primary Carechyntia eryonza100% (1)
- Effect of Ursodeoxycholic Acid On Indirect Hyperbilirubinemia in Neonates Treated With PhototherapyDocument4 pagesEffect of Ursodeoxycholic Acid On Indirect Hyperbilirubinemia in Neonates Treated With PhototherapyEka Satria AnanditaNo ratings yet
- Fluid Management: Suparto Anesthesia Department Medical Faculty Christian Krida Wacana UniversityDocument61 pagesFluid Management: Suparto Anesthesia Department Medical Faculty Christian Krida Wacana UniversitygozaNo ratings yet
- Ventilasi Mekanik Untuk Neonatus: Dr. R. Adhi Teguh Perma Iskandar Sp.A Divisi Perinatologi FKUI-RSCMDocument52 pagesVentilasi Mekanik Untuk Neonatus: Dr. R. Adhi Teguh Perma Iskandar Sp.A Divisi Perinatologi FKUI-RSCMireneaureliaNo ratings yet
- Patent Ductus ArteriosusDocument4 pagesPatent Ductus ArteriosusseigelysticNo ratings yet
- Surfactant ReplacementDocument40 pagesSurfactant ReplacementDr.Sushree Smita BehuraNo ratings yet
- Clinics in Pediatrics: Growth Faltering: The New and The OldDocument10 pagesClinics in Pediatrics: Growth Faltering: The New and The OldJayantiNo ratings yet
- Early Diagnostic Markers For Neonatal Sepsis Comparing Procalcitonin (PCT) and C-Reactive Protein (CRP)Document5 pagesEarly Diagnostic Markers For Neonatal Sepsis Comparing Procalcitonin (PCT) and C-Reactive Protein (CRP)IqbalNo ratings yet
- Rheumatic FeverDocument19 pagesRheumatic FeverKanwal SafeerNo ratings yet
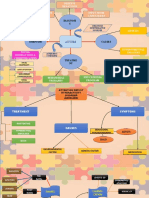
- Mind MapDocument3 pagesMind MapaziemNo ratings yet
- Introduction - Prof SudigdoDocument49 pagesIntroduction - Prof Sudigdoyulia fatma nstNo ratings yet
- Faltering Growth: Straight To The Point of CareDocument35 pagesFaltering Growth: Straight To The Point of Careftah ahmedNo ratings yet
- PEDSQL Generic N CancerDocument17 pagesPEDSQL Generic N CancerJimmy Oi SantosoNo ratings yet
- Pain in Children: Advances & Ongoing ChallengesDocument26 pagesPain in Children: Advances & Ongoing ChallengesDeepak SolankiNo ratings yet
- Hamed2016Document4 pagesHamed2016Franknanda D'enzieroX-zhirawaxaveriuz PutrascreamoDark-nataseNo ratings yet
- PANCE ReviewDocument2 pagesPANCE ReviewFlora LawrenceNo ratings yet
- Penggunaan Sedasi Pada Anak Dengan VentilatorDocument5 pagesPenggunaan Sedasi Pada Anak Dengan VentilatorCalvin AffendyNo ratings yet
- 04 Prof DR Cissy Vaksin Untuk Mencegah Pneumonia Pneumokokus - ColourDocument40 pages04 Prof DR Cissy Vaksin Untuk Mencegah Pneumonia Pneumokokus - ColourYuuki Putri HidayatNo ratings yet
- Golden OurDocument89 pagesGolden OurRosmauliana DamanikNo ratings yet
- Graves' Disease & PregnancyDocument19 pagesGraves' Disease & Pregnancyrajan kumar100% (1)
- Antiepileptic Drugs Continuum 2016Document25 pagesAntiepileptic Drugs Continuum 2016Habib G. Moutran BarrosoNo ratings yet
- Managing Tuberculosis in PregnancyDocument1 pageManaging Tuberculosis in PregnancyAndi Tenri Ola Oddang IINo ratings yet
- BBLRDocument37 pagesBBLRHernina OktavianiNo ratings yet
- Medication, Toxic, and Vitamin-Related NeuropathiesDocument22 pagesMedication, Toxic, and Vitamin-Related Neuropathiessatyagraha84No ratings yet
- Kaufmann PlenaryDocument44 pagesKaufmann Plenaryapi-216587414No ratings yet
- PCOS Guidelines 1Document14 pagesPCOS Guidelines 1Angelie Therese ChuaNo ratings yet
- Congenital Tuberculosis A Review ArticleDocument5 pagesCongenital Tuberculosis A Review ArticleMasita RochsalehaNo ratings yet
- CEBM Levels of EvidenceDocument2 pagesCEBM Levels of EvidenceBellatriix Bonisa MadarjaNo ratings yet
- Rational Blood Transfusion in Infant and ChildrenDocument37 pagesRational Blood Transfusion in Infant and ChildrenBayu KurniawanNo ratings yet
- Childhood Wheezing Approach GuideDocument25 pagesChildhood Wheezing Approach GuideshahinaNo ratings yet
- Psychiatry: A Case Analysis in Course IntegrationDocument40 pagesPsychiatry: A Case Analysis in Course IntegrationMcleo OaferinaNo ratings yet
- Antibiotic Use in Critical Care: DR Radha Sundaram Lead Clinician RAH PaisleyDocument36 pagesAntibiotic Use in Critical Care: DR Radha Sundaram Lead Clinician RAH PaisleyHidayati IdaNo ratings yet
- What Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)Document39 pagesWhat Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)laurentiaNo ratings yet
- Infective EndocarditisDocument66 pagesInfective EndocarditisMulia RahmansyahNo ratings yet
- Non Invasive Ventilation in PediatricsDocument192 pagesNon Invasive Ventilation in Pediatricstj1983tj0% (1)
- Pediatric Normal ValueDocument4 pagesPediatric Normal ValueyaniarsusinNo ratings yet
- Guided by Asso Prof DR Sunil K Agarawalla Presented by DR Minakhi Kumari Sahu (JR-1)Document45 pagesGuided by Asso Prof DR Sunil K Agarawalla Presented by DR Minakhi Kumari Sahu (JR-1)Gobinda Pradhan100% (1)
- Understanding Cerebral PalsyDocument22 pagesUnderstanding Cerebral PalsyJay SorianoNo ratings yet
- Executive Summary: ACCP Evidence-Based Diagnosis and Management of CoughDocument33 pagesExecutive Summary: ACCP Evidence-Based Diagnosis and Management of CoughNitesh GuptaNo ratings yet
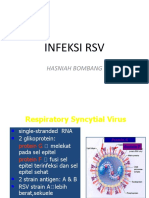
- Infeksi RSV: Hasniah BombangDocument12 pagesInfeksi RSV: Hasniah Bombangmuh hardiansyahNo ratings yet
- ECG Symcard 2016 - Electrocardiography On Congenital Heart Disease PDFDocument53 pagesECG Symcard 2016 - Electrocardiography On Congenital Heart Disease PDFCia100% (1)
- Critical Appraisal RCTDocument7 pagesCritical Appraisal RCTAisya FikritamaNo ratings yet
- Mengenal Resusitasi Pada Anak Dan Bayi Bagi Perawat PemulaDocument15 pagesMengenal Resusitasi Pada Anak Dan Bayi Bagi Perawat PemulaSiti Krisan WijayaNo ratings yet
- Diarrhea in ChildrenDocument42 pagesDiarrhea in ChildrenIPNATC NEPALNo ratings yet
- Patof Spell PDFDocument3 pagesPatof Spell PDFAnggi CalapiNo ratings yet
- RC - PedsQL Infant All - Eng USoriDocument12 pagesRC - PedsQL Infant All - Eng USoriAlma Aparicio67% (3)
- Complete Atrioventricular Canal (CAVC)Document4 pagesComplete Atrioventricular Canal (CAVC)vivid1980No ratings yet
- Anemia PregnancyDocument122 pagesAnemia PregnancySenthil NathNo ratings yet
- Abdominal TuberculosisDocument12 pagesAbdominal TuberculosisBimlesh ThakurNo ratings yet
- Maternal Pocket Book PDFDocument480 pagesMaternal Pocket Book PDFerwina nur100% (1)
- Intravenous Fluid Therapy in Critically Ill AdultsDocument17 pagesIntravenous Fluid Therapy in Critically Ill AdultsntnquynhproNo ratings yet
- Pedsql Module CardioDocument31 pagesPedsql Module CardioRatna100% (1)
- Probiotics:: A "New" Approach To Gastrointestinal Health and DiseaseDocument62 pagesProbiotics:: A "New" Approach To Gastrointestinal Health and DiseaseFelix PradanaNo ratings yet
- Fast Hugs BidDocument1 pageFast Hugs Bidnuttela ismeNo ratings yet
- Pain ManagementDocument39 pagesPain Managementsteven saputra100% (1)
- Acute Pain: Dr. I Putu Pramana Suarjaya, Span. Mkes. KMNDocument35 pagesAcute Pain: Dr. I Putu Pramana Suarjaya, Span. Mkes. KMNAdhi WiratmaNo ratings yet
- PAC Obstetrics ClerkingDocument48 pagesPAC Obstetrics ClerkingAhmad Mustaqim SulaimanNo ratings yet
- Click To Edit Master Title StyleDocument5 pagesClick To Edit Master Title StyleRiyyan InsaniNo ratings yet
- Order SOL Beauty REPORT TEMPLATEDocument1 pageOrder SOL Beauty REPORT TEMPLATEFarhana Fefe Amani FeFeNo ratings yet
- Nur Farhana Amani Absensi HarianDocument2 pagesNur Farhana Amani Absensi HarianFarhana Fefe Amani FeFeNo ratings yet
- Breakfast Recipes FINALDocument20 pagesBreakfast Recipes FINALFazil Duraman75% (4)
- Lecture Notes Clinical AnaesthesiaDocument176 pagesLecture Notes Clinical AnaesthesiaKevinEustaquioNo ratings yet
- Pain Management in Daily Practice For Primary Care: Dr. Suparto, SP - AnDocument38 pagesPain Management in Daily Practice For Primary Care: Dr. Suparto, SP - AnFarhana Fefe Amani FeFeNo ratings yet
- Kelainan Kulit Bawaan:Setelah Lahir: Nur Farhana Amani Binti Che Wan AhmadDocument37 pagesKelainan Kulit Bawaan:Setelah Lahir: Nur Farhana Amani Binti Che Wan AhmadFarhana Fefe Amani FeFeNo ratings yet
- Comparison of Diffractive and Refractive Multifocal Intraocular Lenses in Presbyopia TreatmentDocument5 pagesComparison of Diffractive and Refractive Multifocal Intraocular Lenses in Presbyopia TreatmentFarhana Fefe Amani FeFeNo ratings yet
- Jurnal Baru 1Document9 pagesJurnal Baru 1Farhana Fefe Amani FeFeNo ratings yet
- Fefe Notes Harpini 2Document3 pagesFefe Notes Harpini 2Farhana Fefe Amani FeFeNo ratings yet
- PenilaianstatusgizibalitaantropometriDocument33 pagesPenilaianstatusgizibalitaantropometriFarhana Fefe Amani FeFeNo ratings yet
- Otolaryngology and Anatomy ReferencesDocument1 pageOtolaryngology and Anatomy ReferencesFarhana Fefe Amani FeFeNo ratings yet
- Referat Hiv Aids Cover PageDocument4 pagesReferat Hiv Aids Cover PageFarhana Fefe Amani FeFeNo ratings yet
- Kuliah IpdDocument2 pagesKuliah IpdFarhana Fefe Amani FeFeNo ratings yet
- AARC Clinical Practice Guideline: Static Lung Volumes: 2001 Revision & UpdateDocument9 pagesAARC Clinical Practice Guideline: Static Lung Volumes: 2001 Revision & UpdateFarhana Fefe Amani FeFeNo ratings yet
- Cover Laporan KasusDocument1 pageCover Laporan KasusFarhana Fefe Amani FeFeNo ratings yet
- Retrocaval Ureter Is A Rare Congenital Urologic Anomaly - En.idDocument25 pagesRetrocaval Ureter Is A Rare Congenital Urologic Anomaly - En.idFarhana Fefe Amani FeFeNo ratings yet
- Breakfast Recipes FINALDocument20 pagesBreakfast Recipes FINALFazil Duraman75% (4)
- Nephrotic Syndrome::one of The Clinical Syndromes With Many Causes and Many Histologic AbnormalitiesDocument8 pagesNephrotic Syndrome::one of The Clinical Syndromes With Many Causes and Many Histologic AbnormalitiesFarhana Fefe Amani FeFeNo ratings yet
- Referat Sle Cover PageDocument3 pagesReferat Sle Cover PageFarhana Fefe Amani FeFeNo ratings yet
- Triage - ARDS (Autosaved)Document35 pagesTriage - ARDS (Autosaved)Farhana Fefe Amani FeFeNo ratings yet
- Otolaryngology and Anatomy ReferencesDocument1 pageOtolaryngology and Anatomy ReferencesFarhana Fefe Amani FeFeNo ratings yet
- Lung VolumesDocument2 pagesLung VolumesFarhana Fefe Amani FeFeNo ratings yet
- Dirty Genes Course Copy 1Document181 pagesDirty Genes Course Copy 1Rachel Bruce50% (4)
- DokumenDocument3 pagesDokumenFkep2015No ratings yet
- 10th MSS CPC Clinical AbstractDocument4 pages10th MSS CPC Clinical Abstractregadel07No ratings yet
- Abg Interpretation 2Document1 pageAbg Interpretation 2Barbara Casqueira100% (2)
- Peri Implant Health: Mauricio G. Araujo - Jan LindheDocument7 pagesPeri Implant Health: Mauricio G. Araujo - Jan LindheCristian CulcitchiNo ratings yet
- Sleep Disordered Breathing: Ramon Alcira, MD, FPSO-HNSDocument3 pagesSleep Disordered Breathing: Ramon Alcira, MD, FPSO-HNSMaikka IlaganNo ratings yet
- Uncontrolled Cell DivisionDocument51 pagesUncontrolled Cell Divisionm43No ratings yet
- OSCHMANDocument7 pagesOSCHMANapi-3708784100% (1)
- Brain Herniation SyndromeDocument28 pagesBrain Herniation SyndromeSarahScandy100% (4)
- Language and BrainDocument23 pagesLanguage and Brainalbino100% (1)
- How Ketone Bodies Fuel Brain and HeartDocument3 pagesHow Ketone Bodies Fuel Brain and Heartdaef32No ratings yet
- Pregnant woman with painful swollen legDocument12 pagesPregnant woman with painful swollen legjimmojonesNo ratings yet
- Ayurveda Physical BodyDocument11 pagesAyurveda Physical BodyanantNo ratings yet
- Surgical Resection of Cancer of The Buccal MucosaDocument21 pagesSurgical Resection of Cancer of The Buccal MucosapradeepNo ratings yet
- Characterizing The Subtype of Anhedonia in Major Depressive DisorderDocument9 pagesCharacterizing The Subtype of Anhedonia in Major Depressive DisorderGkani ChrysoulaNo ratings yet
- Hillside School: Biology For Grade 12 Note 2 Topic: The Structure and Function of Bacterial CellDocument8 pagesHillside School: Biology For Grade 12 Note 2 Topic: The Structure and Function of Bacterial Celloli JrNo ratings yet
- NLS InfographicsDocument6 pagesNLS InfographicsMihai Ion GhioaldaNo ratings yet
- 1 - OB 1 (Maternal Anatomy)Document13 pages1 - OB 1 (Maternal Anatomy)Gen XNo ratings yet
- Absolute and Relative Contraindications To IV Rt-PA For Acute Ischemic StrokeDocument12 pagesAbsolute and Relative Contraindications To IV Rt-PA For Acute Ischemic Strokeأبو أويس شرف الدينNo ratings yet
- 3hr Mitosis KahootDocument37 pages3hr Mitosis Kahootapi-283244059No ratings yet
- Neuroparasitology PDFDocument62 pagesNeuroparasitology PDFpsetoNo ratings yet
- Autopsy Report: DECEDENT: John AndersonDocument5 pagesAutopsy Report: DECEDENT: John AndersonjilliankadNo ratings yet
- Organic Molecules: Chapter 2-3Document33 pagesOrganic Molecules: Chapter 2-3Gissele AbolucionNo ratings yet
- Learning Theories of PersonalityDocument13 pagesLearning Theories of Personalitypavitra_madhusudanNo ratings yet
- Benign Diseases of ThyroidDocument70 pagesBenign Diseases of ThyroidMounica MekalaNo ratings yet
- Journey Through DigestionDocument4 pagesJourney Through DigestionJoy JonesNo ratings yet
- Pedia2 Sepsis (Dr. Seng)Document3 pagesPedia2 Sepsis (Dr. Seng)Tony DawaNo ratings yet
- Who Needs Bypass SurgeryDocument70 pagesWho Needs Bypass SurgerymikikiNo ratings yet
- Introduction To Fitness TrainingDocument25 pagesIntroduction To Fitness TrainingShailendra Singh ChouhanNo ratings yet
- Limbic System (Behaviour and Emotion)Document19 pagesLimbic System (Behaviour and Emotion)Patterson MachariaNo ratings yet