You might also like
- Case StudyDocument15 pagesCase Studyapi-589548099No ratings yet
- Schizo PhreniaDocument9 pagesSchizo PhreniaCharles IppolitoNo ratings yet
- 2016 Apego Malaga PDFDocument91 pages2016 Apego Malaga PDFDavid BoixNo ratings yet
- Psychodynamic Concept Map For Bipolar I, ManicDocument1 pagePsychodynamic Concept Map For Bipolar I, ManicShereen ManabilangNo ratings yet
- Psych Ch. 5 NotesDocument7 pagesPsych Ch. 5 NotesHaylle ThomasNo ratings yet
- Coherence Therapy (Previously, Depth-Oriented Brief Therapy)Document13 pagesCoherence Therapy (Previously, Depth-Oriented Brief Therapy)Paola AlarcónNo ratings yet
- Dissociative Identity Disorder in ArtDocument5 pagesDissociative Identity Disorder in ArtsiancampbellNo ratings yet
- Dr. Radhakrishnan G. Assistant Professor & Mrs. K.Sugavanaselvi, Ph.D. ScholarDocument6 pagesDr. Radhakrishnan G. Assistant Professor & Mrs. K.Sugavanaselvi, Ph.D. ScholarnagarajanNo ratings yet
- Tourette Syndrome Research PaperDocument7 pagesTourette Syndrome Research PaperAtme SmileNo ratings yet
- Eating Disorders Reading AssignmentDocument2 pagesEating Disorders Reading AssignmentNasratullah sahebzadaNo ratings yet
- Introduction-: Post Traumatic Stress Disorder (PTSD)Document10 pagesIntroduction-: Post Traumatic Stress Disorder (PTSD)preeti sharmaNo ratings yet
- The Psychiatric Mental Status Exam (MSE)Document4 pagesThe Psychiatric Mental Status Exam (MSE)dev100% (1)
- SSRI (Selective Serotonin Reuptake Inhibitor)Document1 pageSSRI (Selective Serotonin Reuptake Inhibitor)Mike EveretteNo ratings yet
- Delirium, Dementia, PsychosisDocument2 pagesDelirium, Dementia, PsychosisLagente EstalocaNo ratings yet
- Chapter 21 Antidepressant AgentsDocument4 pagesChapter 21 Antidepressant AgentsNicolle Lisay IlaganNo ratings yet
- Tourette'S Disorder: Presented byDocument14 pagesTourette'S Disorder: Presented byjaydipNo ratings yet
- Dance/movement Therapy and Bulimia NervosaDocument89 pagesDance/movement Therapy and Bulimia Nervosaalriboh100% (1)
- Lecture Notes For Mental Health Nursing Psych NursingDocument88 pagesLecture Notes For Mental Health Nursing Psych Nursingjg369097100% (1)
- Use of Flash Technique On A GroupDocument1 pageUse of Flash Technique On A GroupElisa ValdésNo ratings yet
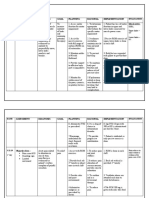
- Nursing Care Plan: Assessment Diagnosis Goal Planning Rational Implementation Objective DataDocument8 pagesNursing Care Plan: Assessment Diagnosis Goal Planning Rational Implementation Objective DataMoonNo ratings yet
- Neurotransmitters: A. Paracrine Regulators (Tissue Hormones)Document11 pagesNeurotransmitters: A. Paracrine Regulators (Tissue Hormones)Prasana100% (1)
- ConversionPsychiatric Symptoms and Dissociation in Conversion, Somatization and Dissociative Disorders15Document7 pagesConversionPsychiatric Symptoms and Dissociation in Conversion, Somatization and Dissociative Disorders15Amir MirzaNo ratings yet
- The Psychology of Gender: PSYC-362-DL1 Taught By: Jason Feinberg Welcome!Document58 pagesThe Psychology of Gender: PSYC-362-DL1 Taught By: Jason Feinberg Welcome!uhhhhNo ratings yet
- Cognitive Disorders PresentationDocument70 pagesCognitive Disorders PresentationWasiu AfoloabiNo ratings yet
- Electro Convulsive Therapy: by Ms. Deepika.K, M.SC (N) - I Year, Dept of Psychiatric Nursing, KGNCDocument24 pagesElectro Convulsive Therapy: by Ms. Deepika.K, M.SC (N) - I Year, Dept of Psychiatric Nursing, KGNCNaveen RajaduraiNo ratings yet
- Algorithm for Treating DepressionDocument12 pagesAlgorithm for Treating Depressioniwul kiwul KriwulNo ratings yet
- ECTDocument24 pagesECTEdgar ManoodNo ratings yet
- What To Know On The Exam: Mania - 7 QuestionsDocument11 pagesWhat To Know On The Exam: Mania - 7 QuestionsNyein Nu WinnNo ratings yet
- Defining Psychological Interventions and Their EffectivenessDocument26 pagesDefining Psychological Interventions and Their EffectivenessJay Mark Cabrera100% (1)
- Case 2Document8 pagesCase 2Kreshnik IdrizajNo ratings yet
- EMDR en PsicooncologíaDocument16 pagesEMDR en PsicooncologíaBelén PicadoNo ratings yet
- Drug List PsychopharmDocument23 pagesDrug List PsychopharmGeorge HananiaNo ratings yet
- CatDocument12 pagesCatnini345No ratings yet
- NeurotransmittersDocument1 pageNeurotransmittersmegs13045No ratings yet
- Hamilton Rating Scale For Anxiety (HAM-A) : Questionnaire ReviewDocument1 pageHamilton Rating Scale For Anxiety (HAM-A) : Questionnaire ReviewIntanwatiNo ratings yet
- BEHAVIOR THERAPY Assignment MSCDocument9 pagesBEHAVIOR THERAPY Assignment MSCannuNo ratings yet
- Psychotherapy TypesDocument36 pagesPsychotherapy TypessilencedurevesNo ratings yet
- Post Traumatic Stress Stress Disorder: by MR - Loganathan.N Lecturer M.SC (Mental Health Nursing)Document28 pagesPost Traumatic Stress Stress Disorder: by MR - Loganathan.N Lecturer M.SC (Mental Health Nursing)Galina StupelimanNo ratings yet
- Understanding Post Traumatic Stress DisorderDocument22 pagesUnderstanding Post Traumatic Stress DisorderPrakriti SharmaNo ratings yet
- CASE PRESENTATION PP - Anxiety. Tiffany GordonDocument6 pagesCASE PRESENTATION PP - Anxiety. Tiffany GordonTiffany GordonNo ratings yet
- Geriatric Depression ScaleDocument2 pagesGeriatric Depression ScaleJess RitumaltaNo ratings yet
- Geriatrics: Care of the ElderlyDocument45 pagesGeriatrics: Care of the ElderlySree Latha100% (1)
- Drug Analysis in PsychDocument3 pagesDrug Analysis in PsychBryan Andrew GonzalesNo ratings yet
- Insomnia PowerpointDocument16 pagesInsomnia Powerpointapi-255944865No ratings yet
- Lifestyle Management FormsDocument41 pagesLifestyle Management Formshearnsbergerbetsy50% (2)
- Anti Psychotic DrugsDocument67 pagesAnti Psychotic DrugsAhmed Osman100% (1)
- Bipolar DisorderDocument4 pagesBipolar DisorderISHIKA SAHANo ratings yet
- Assessment of Personality DisorderDocument9 pagesAssessment of Personality DisorderTauqeer AhmedNo ratings yet
- Bateman Fonagy 2008 Mentalization Based Treatment For BPDDocument16 pagesBateman Fonagy 2008 Mentalization Based Treatment For BPDCamila Piña SanhuezaNo ratings yet
- clinical case studyDocument17 pagesclinical case studyapi-741088437No ratings yet
- Case StudyDocument13 pagesCase Studyapi-599558477No ratings yet
- Comprehensive Case Study MH - SantucciDocument15 pagesComprehensive Case Study MH - Santucciapi-663034532No ratings yet
- DocumentDocument11 pagesDocumentFairuds MamalintaNo ratings yet
- mental health case studyDocument13 pagesmental health case studyapi-731293150No ratings yet
- Psych Careplan For PaperDocument18 pagesPsych Careplan For PaperUSMCDOC100% (2)
- Psychiatric Mental Health Comp Case StudyDocument15 pagesPsychiatric Mental Health Comp Case Studyapi-663431559No ratings yet
- MH Case Study - Whiley DrymonDocument13 pagesMH Case Study - Whiley Drymonapi-664257988No ratings yet
- Case Gynecomastia During Paroxetine TherapyDocument4 pagesCase Gynecomastia During Paroxetine TherapyAhmed Abd El FattahNo ratings yet
- psychiatric mental health comprehensive case studyDocument12 pagespsychiatric mental health comprehensive case studyapi-741551545No ratings yet
- 1.2 Overview & OutcomesDocument9 pages1.2 Overview & OutcomesShayla HudsonNo ratings yet
- Gnrs 556 Cduc Prep Assignment SkinDocument2 pagesGnrs 556 Cduc Prep Assignment Skinapi-437250138No ratings yet
- Cduc Gnrs 588 Comprehensive Care Plan 1Document20 pagesCduc Gnrs 588 Comprehensive Care Plan 1api-437250138No ratings yet
- Gnrs 504 Cduc Zlue Justice Case StudyDocument15 pagesGnrs 504 Cduc Zlue Justice Case Studyapi-437250138No ratings yet
- Gnrs 508a Cduc Bgeo Rkel Zlue Team Assignment G Research Proposal Project PresentationDocument16 pagesGnrs 508a Cduc Bgeo Rkel Zlue Team Assignment G Research Proposal Project Presentationapi-437250138No ratings yet
- Gnrs 508a Cduc Bgeo Rkel Zlue Team Assignment G Research Proposal Project PresentationDocument16 pagesGnrs 508a Cduc Bgeo Rkel Zlue Team Assignment G Research Proposal Project Presentationapi-437250138No ratings yet
- Cduc Cwhi Jcas Rale Gnrs 586 Qi PresentationDocument11 pagesCduc Cwhi Jcas Rale Gnrs 586 Qi Presentationapi-437250138No ratings yet
- Gnrs 508a Cduc Bgeo Rkel Zlue Team Assignment B Analysis and Evaluation of A Nursing Middle Range Theory or Nursing ModelDocument16 pagesGnrs 508a Cduc Bgeo Rkel Zlue Team Assignment B Analysis and Evaluation of A Nursing Middle Range Theory or Nursing Modelapi-437250138No ratings yet
- Inform Es AgendaDocument7 pagesInform Es AgendaArendy Rodríguez SosaNo ratings yet
- Pe-4 GR12 2ndsem 3RDQ Module 3 W5W6Document15 pagesPe-4 GR12 2ndsem 3RDQ Module 3 W5W6Leslie Joy Yata MonteroNo ratings yet
- Nebosh: Management of Health and Safety Unit Ig1Document5 pagesNebosh: Management of Health and Safety Unit Ig1Muhammad Talha0% (1)
- Wilfredo Mallari Resume Safety Supervisor UpdatedDocument1 pageWilfredo Mallari Resume Safety Supervisor Updatedwilly mallariNo ratings yet
- Nutritional Management of Short Bowel Syndrome PDFDocument10 pagesNutritional Management of Short Bowel Syndrome PDFSonya YunitaNo ratings yet
- Natural Pregnancy and ParentingDocument70 pagesNatural Pregnancy and ParentingAmela SabicNo ratings yet
- Block M2 EYE Distribution by MMCDocument3 pagesBlock M2 EYE Distribution by MMCF ParikhNo ratings yet
- Two Step TSTDocument2 pagesTwo Step TSTBrianHoNo ratings yet
- STIs O & GDocument59 pagesSTIs O & GNoraNo ratings yet
- Gastroenterology - Pancreatitis PDFDocument2 pagesGastroenterology - Pancreatitis PDFMonica J Ortiz PereiraNo ratings yet
- Vaishali Bujad Project..2Document54 pagesVaishali Bujad Project..2Mitesh Prajapati 7765No ratings yet
- Quality Control Circle - Desk File and WorkDocument26 pagesQuality Control Circle - Desk File and WorkZuhairi MohamedNo ratings yet
- Training After 40 - Guide To Building and Maintaining A Healthier Leaner and Stronger BodyDocument108 pagesTraining After 40 - Guide To Building and Maintaining A Healthier Leaner and Stronger BodyAnonymous FjHHlskcT100% (6)
- A 10-Year Review of Colonoscopy at Aminu Kano Teaching Hospital, Kano NigeriaDocument5 pagesA 10-Year Review of Colonoscopy at Aminu Kano Teaching Hospital, Kano NigeriaYUSUF MUSANo ratings yet
- DMSCO Log Book Vol.40 1962Document73 pagesDMSCO Log Book Vol.40 1962Des Moines University Archives and Rare Book RoomNo ratings yet
- Furosemide Drug ProfileDocument34 pagesFurosemide Drug ProfileNur Ilmi SofiahNo ratings yet
- Obstetrics 4Document9 pagesObstetrics 4Darrel Allan MandiasNo ratings yet
- 485 5032 Assignment 1 Greenwich University PassDocument27 pages485 5032 Assignment 1 Greenwich University PassThy ThơNo ratings yet
- What Is SalmonellaDocument4 pagesWhat Is SalmonellaRosNo ratings yet
- LUTSDocument9 pagesLUTSHatem SadekNo ratings yet
- Careers in Social Work: Outlook, Pay & MoreDocument9 pagesCareers in Social Work: Outlook, Pay & Morejoel lacayNo ratings yet
- Care Plan Handbook TemplateDocument34 pagesCare Plan Handbook TemplateBreanna Hopkins100% (1)
- Enhancing Your Skills in Stroke Quality Improvement and Data AnalysisDocument50 pagesEnhancing Your Skills in Stroke Quality Improvement and Data AnalysisRaisha Klinik Vaksinasi YogyakartaNo ratings yet
- Pi 021 2 Aide Memoire On GMP GCPDocument10 pagesPi 021 2 Aide Memoire On GMP GCPIsmail MathakiyaNo ratings yet
- Approaches To The Diagnosis of Portal HipertensionDocument12 pagesApproaches To The Diagnosis of Portal HipertensionValentina IorgaNo ratings yet
- Neurorobotics Presentation 3Document8 pagesNeurorobotics Presentation 3Hamza MinhasNo ratings yet
- Body Mass IndexDocument3 pagesBody Mass IndexSunnyVermaNo ratings yet
- Child Development MilestonesDocument6 pagesChild Development Milestonesj_______________jNo ratings yet
- Pediatric Schedule 3Document12 pagesPediatric Schedule 3Luis NepomucenoNo ratings yet
- Hospital Department and UnitDocument30 pagesHospital Department and UnitDwi FebriantoNo ratings yet