You might also like
- Rhinosinusitis PDFDocument14 pagesRhinosinusitis PDFSekarrini VidyatamiNo ratings yet
- Pathogenesis and Diagnosis of Anti-GBM Antibody (Goodpasture's) DiseaseDocument18 pagesPathogenesis and Diagnosis of Anti-GBM Antibody (Goodpasture's) DiseaseDicky SangadjiNo ratings yet
- Mallory Weiss TearDocument12 pagesMallory Weiss TeararshadmunNo ratings yet
- LaporanDocument5 pagesLaporanAgus SusantoNo ratings yet
- Karies GigiDocument5 pagesKaries GigiBian Rahmadi MedikantoNo ratings yet
- Interpretasi EKG Claudio Per 14 April 2019Document39 pagesInterpretasi EKG Claudio Per 14 April 2019Claudio AgustinoNo ratings yet
- Fraktur Dan Infeksi TulangDocument25 pagesFraktur Dan Infeksi TulangAnonymous HAbhRTs2TfNo ratings yet
- Pityriasis Rosea - Background, Pathophysiology, EtiologyDocument4 pagesPityriasis Rosea - Background, Pathophysiology, EtiologysyahrulroziNo ratings yet
- Lesi Osteolitic Costa 6 Belakang S Lesi Osteoblastic Costa 6-7 Belakang DDocument48 pagesLesi Osteolitic Costa 6 Belakang S Lesi Osteoblastic Costa 6-7 Belakang DLusi MunawarohNo ratings yet
- CR Piopneumothoraks Nicky FIXdDocument62 pagesCR Piopneumothoraks Nicky FIXdPutri RahmawatiNo ratings yet
- Paederus Dermatitis Karthikeyan K, Kumar A - Indian J Dermatol Venereol LeprolDocument11 pagesPaederus Dermatitis Karthikeyan K, Kumar A - Indian J Dermatol Venereol Leprolalmas prawoto100% (1)
- A Clinical Study of Etiology and Management of Acute Intestinal ObstructionDocument6 pagesA Clinical Study of Etiology and Management of Acute Intestinal ObstructionFalon PapalangiNo ratings yet
- Jurnal Reading: Pembimbing: DR - Erna M Marbun, SPTHTDocument7 pagesJurnal Reading: Pembimbing: DR - Erna M Marbun, SPTHTJessica LawrenceNo ratings yet
- Erin's Rad ReviewDocument111 pagesErin's Rad ReviewmadamzelleyNo ratings yet
- Sindrom NefrotikDocument22 pagesSindrom NefrotikGyta Apriati100% (1)
- Drug EruptionDocument46 pagesDrug EruptionSisca ChearzNo ratings yet
- KARDIOMYOPATI - Kuliah DR - ErlinaDocument28 pagesKARDIOMYOPATI - Kuliah DR - ErlinaArif Zulfian MubarokNo ratings yet
- CR DR - Dedi Hidropneumothorax Ec TB ParuDocument38 pagesCR DR - Dedi Hidropneumothorax Ec TB ParuBunga Listia ParamitaNo ratings yet
- Diabetes Melitus: Dr. Ihsanil Husna, SPPDDocument67 pagesDiabetes Melitus: Dr. Ihsanil Husna, SPPDnathan timothyNo ratings yet
- Taklimat Perubatan Forensik - PENGENALANDocument62 pagesTaklimat Perubatan Forensik - PENGENALANzahariNo ratings yet
- Verview: Scoliosisopen Pop-Up Dialog BoxDocument6 pagesVerview: Scoliosisopen Pop-Up Dialog BoxAnton DeeNo ratings yet
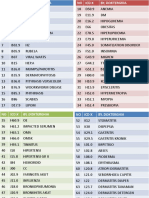
- Icd XDocument3 pagesIcd XR Ghianesya GantinaNo ratings yet
- 25 Chabib Fachry AlbabDocument3 pages25 Chabib Fachry Albabfachry albabNo ratings yet
- K4. Diagnosis Holistik - EngDocument21 pagesK4. Diagnosis Holistik - EngBevila KorspoilvilNo ratings yet
- Management of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientDocument12 pagesManagement of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientRani Dwi NNo ratings yet
- Refreshing Obat Muscle Relaxant AnestesiDocument34 pagesRefreshing Obat Muscle Relaxant AnestesiAnugrah Dwi RiskiNo ratings yet
- TiroidDocument26 pagesTiroidJoni Riana MustaqimNo ratings yet
- Jurnal Reading MataDocument37 pagesJurnal Reading MataAiya Auri GumantiNo ratings yet
- CH 5 Implantation, Placental Dev (Part1)Document36 pagesCH 5 Implantation, Placental Dev (Part1)Tengku Chairannisa PutriNo ratings yet
- Pembahasan To 1 (Patof) Batch Feb 2016Document718 pagesPembahasan To 1 (Patof) Batch Feb 2016ilmupengetahuanNo ratings yet
- Jamur Penyebab Infeksi Respirasi PDFDocument122 pagesJamur Penyebab Infeksi Respirasi PDFdesyNo ratings yet
- Human Papilloma Virus (HPV) (PSPD)Document11 pagesHuman Papilloma Virus (HPV) (PSPD)Sari FitrianingsihNo ratings yet
- Jurnal Forensik Trauma KimiaDocument5 pagesJurnal Forensik Trauma Kimiaikram hanafiNo ratings yet
- Praktikum MalariaDocument22 pagesPraktikum MalariaGeniaaldafitriaasgen100% (1)
- Kuliah 16 Cor PulmonaleDocument41 pagesKuliah 16 Cor PulmonalecaturwiraNo ratings yet
- Algorithm Kel 3Document1 pageAlgorithm Kel 3Anonymous 5zeOnd1No ratings yet
- Komplikasi RhinosinusitisDocument54 pagesKomplikasi RhinosinusitisWilda Kamila SungkarNo ratings yet
- Refleksi Kasus IPE Dan IPECP - Sisilia Dwi Andini Putri 2020401163Document27 pagesRefleksi Kasus IPE Dan IPECP - Sisilia Dwi Andini Putri 2020401163Albinarta YanotamaNo ratings yet
- Systemic Lupus Erythematosus: Pathogenesis and Clinical FeaturesDocument30 pagesSystemic Lupus Erythematosus: Pathogenesis and Clinical FeaturesOrion JohnNo ratings yet
- Palmoplantar PustulosisDocument3 pagesPalmoplantar PustulosisRobby ZayendraNo ratings yet
- MorganDocument14 pagesMorganAdi WijayantoNo ratings yet
- Leptospirosis by DR SarmaDocument37 pagesLeptospirosis by DR SarmaTias Diah0% (1)
- Tifoid PerforasiDocument5 pagesTifoid PerforasiSisca Dwi Agustina0% (1)
- Congenital GlaucomaDocument27 pagesCongenital Glaucomaanon_373532435No ratings yet
- Periappendicular InfiltrateDocument5 pagesPeriappendicular InfiltrateRiz Sanfebrian AdiatmaNo ratings yet
- GestosisDocument12 pagesGestosisravannofanizzaNo ratings yet
- Rin - O24: Cervicitis Gonorhoea (Vietnam Rose) # Nona AsimptomatikDocument6 pagesRin - O24: Cervicitis Gonorhoea (Vietnam Rose) # Nona AsimptomatikNurrahma Putrie HapsariNo ratings yet
- Toxic GasesDocument21 pagesToxic GasesBestariNugrahiniNo ratings yet
- Kajian Interaksi Obat CKDDocument7 pagesKajian Interaksi Obat CKDCinantya Meyta SariNo ratings yet
- Status Epileptikus Morning ReportDocument16 pagesStatus Epileptikus Morning Reportlie antoNo ratings yet
- Status Kalazion - Yoga 1161050136Document10 pagesStatus Kalazion - Yoga 1161050136Yoga WitularNo ratings yet
- Hipertiroid HarrisonDocument8 pagesHipertiroid HarrisonravenskaNo ratings yet
- Partus Spontam Pervaginam FixedDocument29 pagesPartus Spontam Pervaginam FixedRony ArzalNo ratings yet
- Journal ISKDocument4 pagesJournal ISKNova Aditya WijayaNo ratings yet
- CBD Fita DR Ana 123Document67 pagesCBD Fita DR Ana 123Fita Diyan ErikaNo ratings yet
- Case Based Discussion: Oleh: Fita Diyan Erika Pembimbing: Dr. Nur Ana C, Sp. PD, KEMD, FINASIMDocument19 pagesCase Based Discussion: Oleh: Fita Diyan Erika Pembimbing: Dr. Nur Ana C, Sp. PD, KEMD, FINASIMFita Diyan ErikaNo ratings yet
- Morning Report: Dr. Catur Budi K., Sp. PDocument14 pagesMorning Report: Dr. Catur Budi K., Sp. PsherenridcaNo ratings yet
- Case Based Discussion: Supervisor: Dr. Nur Ana C, Sp. PD, KEMD, FINASIMDocument25 pagesCase Based Discussion: Supervisor: Dr. Nur Ana C, Sp. PD, KEMD, FINASIMFita Diyan ErikaNo ratings yet
- Orning Eport: Reported By: Tita - Siti Moderator: Dr. Suyoso, SP - PD Tuesday, November 27 2018Document14 pagesOrning Eport: Reported By: Tita - Siti Moderator: Dr. Suyoso, SP - PD Tuesday, November 27 2018Tita RetnoNo ratings yet
- CBD DR Anna - Aulia Ayu SabillaDocument48 pagesCBD DR Anna - Aulia Ayu SabillaSandra MignonNo ratings yet
- S 019 LBLDocument22 pagesS 019 LBLZenithaMeidaNo ratings yet
- CGJ 18 29Document7 pagesCGJ 18 29ZenithaMeidaNo ratings yet
- CGJ 18 29 PDFDocument6 pagesCGJ 18 29 PDFZenithaMeidaNo ratings yet
- Treatment of Steroid Sensitive Nephrotic Syndrome: A.S. AbeyagunawardenaDocument8 pagesTreatment of Steroid Sensitive Nephrotic Syndrome: A.S. AbeyagunawardenaZenithaMeidaNo ratings yet
- Pathophysiology of OsteoporosisDocument6 pagesPathophysiology of OsteoporosisZenithaMeidaNo ratings yet
- Leukoaraiosis and StrokeDocument5 pagesLeukoaraiosis and StrokeZenithaMeidaNo ratings yet
- Anatomy and Pathophysiology of Stroke: Eitan AurielDocument8 pagesAnatomy and Pathophysiology of Stroke: Eitan AurielZenithaMeidaNo ratings yet
- PX NN CranialDocument35 pagesPX NN CranialZenithaMeidaNo ratings yet
- Bab IDocument4 pagesBab IZenithaMeidaNo ratings yet
- Heart Failure in Pediatric Patients With Congenital Heart DiseaseDocument18 pagesHeart Failure in Pediatric Patients With Congenital Heart DiseaseZenithaMeidaNo ratings yet
- The Past TenseDocument16 pagesThe Past TenseZenithaMeidaNo ratings yet
- What Are Heart Disease and Stroke?Document2 pagesWhat Are Heart Disease and Stroke?ZenithaMeidaNo ratings yet
- Ist2008 PDFDocument6 pagesIst2008 PDFZenithaMeidaNo ratings yet
- 1746 4358 4 13 PDFDocument6 pages1746 4358 4 13 PDFZenithaMeidaNo ratings yet
- Allopurinol and Bone Marrow AplasiaDocument1 pageAllopurinol and Bone Marrow AplasiaZenithaMeidaNo ratings yet
- Rabies Post Exposure Prophylaxis (RPEP) Algorithm: Call County Health DepartmentDocument1 pageRabies Post Exposure Prophylaxis (RPEP) Algorithm: Call County Health DepartmentZenithaMeidaNo ratings yet
- Fluids and Electrolytes ImbalancesDocument7 pagesFluids and Electrolytes Imbalancessinister17No ratings yet
- READINGDocument21 pagesREADINGdiya baby100% (1)
- Gastroenterology and Hepatology Test RequestDocument4 pagesGastroenterology and Hepatology Test Requestbassam alharaziNo ratings yet
- Palliative CareDocument35 pagesPalliative CareChucky Vergara75% (4)
- Haad QuestionDocument20 pagesHaad QuestionNimraj PatelNo ratings yet
- Awareness Knowledge and Attitude About Dengue AmonDocument5 pagesAwareness Knowledge and Attitude About Dengue AmonSachintha PasinduNo ratings yet
- Autsim and Vitamin DDocument4 pagesAutsim and Vitamin DNo OneNo ratings yet
- Heart Rate Variability Biofeedback Increases Baroreflex Gain and Peak Expiratory FlowDocument17 pagesHeart Rate Variability Biofeedback Increases Baroreflex Gain and Peak Expiratory FlowLuis A Gil PantojaNo ratings yet
- Enzymes - What The Experts KnowDocument252 pagesEnzymes - What The Experts KnowRocio Uresti De Ramirez0% (1)
- SGD 3 Case ProtocolDocument2 pagesSGD 3 Case ProtocolJulie Ann TrinidadNo ratings yet
- Panadeine: What Is in This LeafletDocument3 pagesPanadeine: What Is in This Leafletradzi66No ratings yet
- You Don't Have To Be Diabetic To Love This Cookbook 250 Amazing Dishes For People With Diabetes and Their Families and Friends PDFDocument385 pagesYou Don't Have To Be Diabetic To Love This Cookbook 250 Amazing Dishes For People With Diabetes and Their Families and Friends PDFGustavo Eduardo Romero Camarena100% (1)
- DreamsDocument52 pagesDreamsNill SalunkeNo ratings yet
- Pio DermaDocument23 pagesPio Dermabla01No ratings yet
- Spinal Exercise Home ProgrammeDocument19 pagesSpinal Exercise Home ProgrammePrabha VetrichelvanNo ratings yet
- Feletti & Anda, 2010Document23 pagesFeletti & Anda, 2010Mikaela DavisonNo ratings yet
- Neurological Disease in Lupus: Toward A Personalized Medicine ApproachDocument12 pagesNeurological Disease in Lupus: Toward A Personalized Medicine ApproachjerejerejereNo ratings yet
- Alternative Fibromyalgia Pain Management SuggestionsDocument4 pagesAlternative Fibromyalgia Pain Management SuggestionsCinda CrawfordNo ratings yet
- Flu Vaccine: Information For People at RiskDocument8 pagesFlu Vaccine: Information For People at Riskkovi mNo ratings yet
- A Beautiful Mind ReviewDocument9 pagesA Beautiful Mind ReviewPatriciaChristieNo ratings yet
- Kelompok 2 H2S 97-2003 PPT ToksikDocument38 pagesKelompok 2 H2S 97-2003 PPT ToksikHerfando Maulana AlhafizhNo ratings yet
- Eugenical News - 1940 F. K. M. Volume VII 1922-152Document152 pagesEugenical News - 1940 F. K. M. Volume VII 1922-152Keith KnightNo ratings yet
- NP 1 - Board of NursingDocument34 pagesNP 1 - Board of NursingGo IdeasNo ratings yet
- Aztecs and IncasDocument14 pagesAztecs and Incasjamesryan831No ratings yet
- Nash Leaders in TyphoidDocument25 pagesNash Leaders in TyphoidhompatNo ratings yet
- CTG Interpretation of CTG and CFHM During Antepartum and Intrapartum Periods Ho Lai FongDocument33 pagesCTG Interpretation of CTG and CFHM During Antepartum and Intrapartum Periods Ho Lai FongSabrina AzizNo ratings yet
- Approach To ComaDocument33 pagesApproach To ComaDương Đình ThuậnNo ratings yet
- SucralfateDocument3 pagesSucralfateViziteu AlexandraNo ratings yet
- Staffing July 10 12 2022Document5 pagesStaffing July 10 12 2022Kasandra Dawn Moquia BerisoNo ratings yet
- Cardio PDFDocument94 pagesCardio PDFSalwaNo ratings yet