You might also like
- Case ReportDocument57 pagesCase ReportlmandahaNo ratings yet
- Tibia ProximalDocument51 pagesTibia Proximalchenth3r3No ratings yet
- Fracture Tibia & Fibula-1Document111 pagesFracture Tibia & Fibula-1Usaid SulaimanNo ratings yet
- Scapula Fracture Treatment & Management: Author: Thomas P Goss, MD Chief Editor: S Ashfaq Hasan, MDDocument24 pagesScapula Fracture Treatment & Management: Author: Thomas P Goss, MD Chief Editor: S Ashfaq Hasan, MDjohanesNo ratings yet
- Femoral Supracondylar Fractures: Prepared by Dr. Ramzy Sh. ShikhanDocument77 pagesFemoral Supracondylar Fractures: Prepared by Dr. Ramzy Sh. ShikhanRamzi ShukriNo ratings yet
- Conservative Treatment of Diaphyseal Fractures of Tibia andDocument40 pagesConservative Treatment of Diaphyseal Fractures of Tibia andsaihaNo ratings yet
- Lect 8 Lower Extremity Fracture 2Document22 pagesLect 8 Lower Extremity Fracture 220-221 Crisny Novika Yely Br. HutagaolNo ratings yet
- Fracture Shaft Humerus - 030014Document60 pagesFracture Shaft Humerus - 030014MohammedShahidNo ratings yet
- Fractures of The Humeral ShaftDocument25 pagesFractures of The Humeral ShaftMuhammad IqbalNo ratings yet
- Fractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyasDocument90 pagesFractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyaspattiyahNo ratings yet
- ORP - Handout - English - Malleolar FracturesDocument15 pagesORP - Handout - English - Malleolar Fracturesadrian1989No ratings yet
- Musculoskeletal Trauma Cases in Lower Extremities and Its ManagementDocument41 pagesMusculoskeletal Trauma Cases in Lower Extremities and Its ManagementAli AbdullahNo ratings yet
- Classifying and Treating Femoral FracturesDocument28 pagesClassifying and Treating Femoral FracturesNinaNo ratings yet
- Knee Tibia & Ankle InjuriesDocument88 pagesKnee Tibia & Ankle InjuriesNasser AlQadhibNo ratings yet
- Forearm Fracture 1 BismillahDocument17 pagesForearm Fracture 1 Bismillahamel015No ratings yet
- Nursing Management: Musculoskeletal Trauma and Orthopedic SurgeryDocument25 pagesNursing Management: Musculoskeletal Trauma and Orthopedic SurgeryDeannahTampusNo ratings yet
- Lecture 7 Femoral Diapisis and Distal FDocument16 pagesLecture 7 Femoral Diapisis and Distal FQueen SofiaNo ratings yet
- Case Study of "Subtrochanteric Femur": Prepared By: John Ress A. Escobal Group 1Document11 pagesCase Study of "Subtrochanteric Femur": Prepared By: John Ress A. Escobal Group 1J.r. MercadoNo ratings yet
- Clavicle Fracture, SC Joint and Ac Joint Injury: Team IiiDocument19 pagesClavicle Fracture, SC Joint and Ac Joint Injury: Team IiiJunarto Putra TandiarrangNo ratings yet
- Hip FracturesDocument74 pagesHip FracturesMina SamirNo ratings yet
- U04 Fxs of Humeral ShaftDocument88 pagesU04 Fxs of Humeral Shaftadrian_mogosNo ratings yet
- Scapula FracturesDocument24 pagesScapula FracturesFrancesco BenazzoNo ratings yet
- Injury Around The Elbow: Mohamad Afiq Izzuddin 1001336000 Group 3Document51 pagesInjury Around The Elbow: Mohamad Afiq Izzuddin 1001336000 Group 3Star CruiseNo ratings yet
- Elbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsDocument57 pagesElbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsHajar AlSaediNo ratings yet
- Principles of ImmobilizationDocument27 pagesPrinciples of ImmobilizationSivaneasan KandiahNo ratings yet
- Mallet FingerDocument14 pagesMallet FingerMuskan MuhemmedNo ratings yet
- 4 150512145223 Lva1 App6891Document40 pages4 150512145223 Lva1 App6891Rizky HandayaniNo ratings yet
- Pilon FractureDocument49 pagesPilon FractureJinnasit TeeNo ratings yet
- Closed reduction and internal fixation of humerus shaft fractures with Ender nailsDocument56 pagesClosed reduction and internal fixation of humerus shaft fractures with Ender nailsRakesh KumarNo ratings yet
- OPEN FRACTURES Final Dr. Nishith SharmaDocument41 pagesOPEN FRACTURES Final Dr. Nishith SharmaNishith SharmaNo ratings yet
- Coronoid FractureDocument38 pagesCoronoid FractureRamin MaharjanNo ratings yet
- 6-Fractures and Joints Dislocations ManagementDocument91 pages6-Fractures and Joints Dislocations ManagementMUGISHA GratienNo ratings yet
- Fractures HFHDocument74 pagesFractures HFHEmmanuel Papa AcquahNo ratings yet
- Injuries Around The ShoulderDocument81 pagesInjuries Around The ShoulderMisoNo ratings yet
- LowerDocument89 pagesLowerBedo GikryNo ratings yet
- Paediatric FracturesDocument23 pagesPaediatric Fracturesjerry999No ratings yet
- Humeral Shaft Fractures: Nonoperative and Operative Treatment OptionsDocument82 pagesHumeral Shaft Fractures: Nonoperative and Operative Treatment OptionsYoga AninditaNo ratings yet
- Fracture Dan Penanganan EmergencyDocument52 pagesFracture Dan Penanganan Emergencyshindie lethulurNo ratings yet
- Proximal Humeral Fracture Repair and RehabilitationDocument8 pagesProximal Humeral Fracture Repair and RehabilitationAnonymous UClts4nYNo ratings yet
- Tibial PlateauDocument43 pagesTibial Plateauamal.fathullahNo ratings yet
- Ortho PresentationDocument21 pagesOrtho PresentationAkmal ZaibNo ratings yet
- Arthroplasty of Shoulder - MKKPPTXDocument54 pagesArthroplasty of Shoulder - MKKPPTXMis StromNo ratings yet
- Common Lower Limb Fracture: DR Tarif Alakhras Orthopedic Surgeon KFMCDocument49 pagesCommon Lower Limb Fracture: DR Tarif Alakhras Orthopedic Surgeon KFMCahmad albab100% (1)
- Fracture: Suchithra.P.V 1 Year Msc. Nursing College of Nursing AlappuzhaDocument96 pagesFracture: Suchithra.P.V 1 Year Msc. Nursing College of Nursing AlappuzhaAakash A. AgrawalNo ratings yet
- Distal Radial Injury: Department of Orthopaedics SGH Didactic LectureDocument52 pagesDistal Radial Injury: Department of Orthopaedics SGH Didactic Lecturedrscribd1No ratings yet
- 2.supracondylar Humerus FracturesDocument26 pages2.supracondylar Humerus FracturesDabessa MosissaNo ratings yet
- Seminar On Upper Limb FractureDocument166 pagesSeminar On Upper Limb FractureArko dutta100% (1)
- Blue Writing Is What I Added To These Notes: RadiographyDocument46 pagesBlue Writing Is What I Added To These Notes: Radiographybjpalmer100% (2)
- Patellar Fracture 1Document39 pagesPatellar Fracture 1Syafiq ShahbudinNo ratings yet
- Copy of Lower Extremity Bone Fracture Lecture 3Document88 pagesCopy of Lower Extremity Bone Fracture Lecture 3Tselmeg TselmegNo ratings yet
- Lower Limb FracturesDocument124 pagesLower Limb Fracturesmau tau100% (1)
- LisfrancDocument25 pagesLisfrancSamir AsmarNo ratings yet
- Fractures of Shoulder and Elbow EditedDocument25 pagesFractures of Shoulder and Elbow EditedSurgicalgownNo ratings yet
- Malleolar Fractures - Handout PDFDocument14 pagesMalleolar Fractures - Handout PDFAlin Bratu100% (2)
- Lower Limb Fracture..MeDocument142 pagesLower Limb Fracture..MeWorku KifleNo ratings yet
- Clavicle FractureDocument33 pagesClavicle FractureNitin AggarwalNo ratings yet
- Immobilization and Transport On Patient FractureDocument58 pagesImmobilization and Transport On Patient FractureDinaNo ratings yet
- Patellar FractureDocument25 pagesPatellar FractureSyafiq ShahbudinNo ratings yet
- Fractures of The Upper Limb: Dr. Salman AbbasiDocument60 pagesFractures of The Upper Limb: Dr. Salman AbbasiSeimal MahmoodNo ratings yet
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- Open Radical Cholecystectomy With Partial Hepatectomy For Gallbladder CancerDocument2 pagesOpen Radical Cholecystectomy With Partial Hepatectomy For Gallbladder CancerDabessa MosissaNo ratings yet
- Soft Tissue TumorDocument248 pagesSoft Tissue TumorDabessa MosissaNo ratings yet
- Management of Hepatic CystsDocument12 pagesManagement of Hepatic CystsDabessa MosissaNo ratings yet
- Techniques of Exposure, Hilar DissectionDocument20 pagesTechniques of Exposure, Hilar DissectionDabessa MosissaNo ratings yet
- Bone and Joint InfectionsDocument153 pagesBone and Joint InfectionsDabessa MosissaNo ratings yet
- Fractures of The Femoral NeckDocument37 pagesFractures of The Femoral NeckDabessa MosissaNo ratings yet
- Esophageal Perforation TreatmentDocument4 pagesEsophageal Perforation TreatmentDabessa MosissaNo ratings yet
- Whipple ProcedureDocument16 pagesWhipple ProcedureDabessa MosissaNo ratings yet
- General Consideration in EsophagectomyDocument4 pagesGeneral Consideration in EsophagectomyDabessa MosissaNo ratings yet
- External FixatorDocument19 pagesExternal FixatorDabessa MosissaNo ratings yet
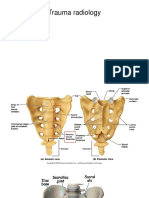
- Trauma RadiologyDocument9 pagesTrauma RadiologyDabessa MosissaNo ratings yet
- Humerous Fxs With Radial Nerve PalsyDocument26 pagesHumerous Fxs With Radial Nerve PalsyDabessa MosissaNo ratings yet
- Common FractureDocument314 pagesCommon FractureDabessa MosissaNo ratings yet
- 2.supracondylar Humerus FracturesDocument26 pages2.supracondylar Humerus FracturesDabessa MosissaNo ratings yet
- Hand IncisionsDocument55 pagesHand IncisionsDabessa Mosissa100% (2)
- Flexor Tendon AnatomyDocument29 pagesFlexor Tendon AnatomyDabessa MosissaNo ratings yet
- Midfoot TraumaDocument26 pagesMidfoot TraumaDabessa MosissaNo ratings yet
- Surgical Approaches and Applied AnatomyDocument44 pagesSurgical Approaches and Applied AnatomyDabessa MosissaNo ratings yet
- The ForearmDocument49 pagesThe ForearmDabessa MosissaNo ratings yet
- Trigger Finger (TF)Document59 pagesTrigger Finger (TF)Dabessa MosissaNo ratings yet
- Trauma RadiologyDocument9 pagesTrauma RadiologyDabessa MosissaNo ratings yet
- Fingertip AmputationDocument41 pagesFingertip AmputationDabessa MosissaNo ratings yet
- The ForearmDocument49 pagesThe ForearmDabessa MosissaNo ratings yet
- Congenital Diaphragmatic HerniaDocument45 pagesCongenital Diaphragmatic HerniaDabessa MosissaNo ratings yet
- EsophagusDocument24 pagesEsophagusDabessa MosissaNo ratings yet
- JaundiceDocument12 pagesJaundiceDabessa MosissaNo ratings yet
- Pediatric Surgical ThemesDocument32 pagesPediatric Surgical ThemesDabessa MosissaNo ratings yet
- Discribd DocumentDocument1 pageDiscribd DocumentDabessa MosissaNo ratings yet
- Discribd DocumentDocument1 pageDiscribd DocumentDabessa MosissaNo ratings yet
- Skeletal System: The Appendicular Skeleton: Clinical Case StudyDocument24 pagesSkeletal System: The Appendicular Skeleton: Clinical Case Studyodiseu81No ratings yet
- Shoulder StretchesDocument11 pagesShoulder StretchesAnna Anna100% (1)
- PNF Techniques in The Upper ExtremityDocument27 pagesPNF Techniques in The Upper ExtremitysanalcrazyNo ratings yet
- ExercíciosDocument2 pagesExercíciosvatomarnocuNo ratings yet
- Management of Primary Anterior Shoulder Dislocations: A Narrative ReviewDocument8 pagesManagement of Primary Anterior Shoulder Dislocations: A Narrative Reviewamal.fathullahNo ratings yet
- 3B Arm Model - M11Document28 pages3B Arm Model - M11rswongym449No ratings yet
- Daniel Garcia - NextDocument18 pagesDaniel Garcia - NextMinh Tô67% (3)
- Upper Limb Mcq PDF FREE DOWNLOADDocument7 pagesUpper Limb Mcq PDF FREE DOWNLOADTendai Chirisa100% (1)
- Techno Card Us PDFDocument48 pagesTechno Card Us PDFROMEOPUNTO67% (3)
- Splint Fabrication Evaluation FormDocument14 pagesSplint Fabrication Evaluation FormJess QuickNo ratings yet
- Exercise Programme PDFDocument25 pagesExercise Programme PDFskhumbuzomadunaNo ratings yet
- Supraspinatus TendinitisDocument7 pagesSupraspinatus Tendinitismilananand100% (1)
- Manus FracturesDocument25 pagesManus FracturesAnonymous 65zjdAVNo ratings yet
- The Silver Dollar System - J. Burke WhittakerDocument83 pagesThe Silver Dollar System - J. Burke Whittakerronmack12100% (3)
- Brachial Plexus MGTDocument30 pagesBrachial Plexus MGTcentrino17100% (2)
- Intro To Ortho Anatomy PDFDocument55 pagesIntro To Ortho Anatomy PDFlanghalilafaNo ratings yet
- Management of Fractures of The Proximal UlnaDocument12 pagesManagement of Fractures of The Proximal UlnaDiana Marcela Benítez HernándezNo ratings yet
- Biceps Brachii Rupture FinalDocument27 pagesBiceps Brachii Rupture Finalapi-282332260No ratings yet
- Wrist Hand Finger ExercisesDocument5 pagesWrist Hand Finger ExercisesNicolae MihaliNo ratings yet
- Single-Stage Reconstruction of Elbow Flexion Associated With Massive Soft-Tissue Defect Using The Latissimus Dorsi Muscle Bipolar Rotational TransferDocument9 pagesSingle-Stage Reconstruction of Elbow Flexion Associated With Massive Soft-Tissue Defect Using The Latissimus Dorsi Muscle Bipolar Rotational TransferSherif HantashNo ratings yet
- Carpal Bones: Sally Left The Party To Take Carol Home Scaphoid, Lunate, Triquetrum (Tri 3)Document1 pageCarpal Bones: Sally Left The Party To Take Carol Home Scaphoid, Lunate, Triquetrum (Tri 3)leahbayNo ratings yet
- 12 Oktober 2017 - Swan Neck Deformity Vs BoutonniereDocument48 pages12 Oktober 2017 - Swan Neck Deformity Vs BoutonniereGerard BennyNo ratings yet
- Kai Greene-Biceps CompressedDocument17 pagesKai Greene-Biceps CompressedYoussef MehrezNo ratings yet
- Suzuki Guitar Vol 4Document17 pagesSuzuki Guitar Vol 4rodrigopatriaNo ratings yet
- 21 JMSCRDocument6 pages21 JMSCRRakesh KumarNo ratings yet
- Section 3 Quiz: Multiple ChoiceDocument2 pagesSection 3 Quiz: Multiple ChoicepoNo ratings yet
- Home Exercise Program For Frozen Shoulder/Adhesive CapsulitisDocument2 pagesHome Exercise Program For Frozen Shoulder/Adhesive CapsulitisRiaz KhanNo ratings yet
- OIA of Cat MusclesDocument8 pagesOIA of Cat Musclesksdfsd8903No ratings yet
- Anatomy McqsDocument2 pagesAnatomy McqsNoor Saleem100% (2)