You might also like
- How To Measure BPDocument25 pagesHow To Measure BPSenen PaezNo ratings yet
- Optimum Way BP 2023Document37 pagesOptimum Way BP 2023herryaptNo ratings yet
- Measuring Blood Pressure: Stella PalarDocument30 pagesMeasuring Blood Pressure: Stella Palarastrid abrahamsNo ratings yet
- BP Measurement BookletDocument13 pagesBP Measurement BookletMohd KhateebNo ratings yet
- Hypertension Prof SyakibDocument78 pagesHypertension Prof SyakibAdibah TajuddinNo ratings yet
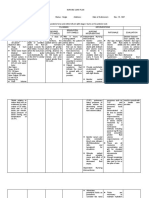
- NCP, DS, GenogramDocument11 pagesNCP, DS, GenogramElva Borlado BilocuraNo ratings yet
- How To Measure Blood Pressure Using A Sphygmomanometer?: Dr. Elmehdawi RR January 2012Document13 pagesHow To Measure Blood Pressure Using A Sphygmomanometer?: Dr. Elmehdawi RR January 2012Magdi Awad SasiNo ratings yet
- Blood Pressure MeasurementDocument2 pagesBlood Pressure MeasurementMaryHope100% (1)
- Proper blood pressure measurement techniqueDocument1 pageProper blood pressure measurement techniqueIoana EcaterinaNo ratings yet
- 1992 - Kaplan - Blood Pressure Measurement and MonitoringDocument33 pages1992 - Kaplan - Blood Pressure Measurement and MonitoringKTKL RSABNo ratings yet
- Medicine - IiDocument22 pagesMedicine - IiMaster MastrikerNo ratings yet
- JNC 7Document12 pagesJNC 7Theresia KennyNo ratings yet
- FNE Anthropometrics Blood Pressure Companion Guide v8Document16 pagesFNE Anthropometrics Blood Pressure Companion Guide v8LeandroNunesAzevedo100% (1)
- Hipertensi JNC 7 VS Hipertensi JNC 8Document99 pagesHipertensi JNC 7 VS Hipertensi JNC 8Sarah Riskita MaizaliusNo ratings yet
- Hypertension Self ManagementDocument23 pagesHypertension Self ManagementElizabeth HoNo ratings yet
- HT 3 PDFDocument24 pagesHT 3 PDFDhen Mas PrimanaNo ratings yet
- ESH Practice Guidelines On Measurement J Hypertens Mar 2005Document5 pagesESH Practice Guidelines On Measurement J Hypertens Mar 2005Cristina StoianNo ratings yet
- Validation of TONOPORT V Blood PressureDocument5 pagesValidation of TONOPORT V Blood PressureAnanta Faxia K WNo ratings yet
- Hypertensive CrisisDocument13 pagesHypertensive CrisisJoanna TaylanNo ratings yet
- Lecture 7. Secondary HypertensionDocument64 pagesLecture 7. Secondary HypertensionkrisnadewirahadiNo ratings yet
- Clinical HypertensionDocument18 pagesClinical Hypertensionsatyajeev soburrunNo ratings yet
- A Pocket Guide To Blood Pressure Measurement in ChildrenDocument4 pagesA Pocket Guide To Blood Pressure Measurement in ChildrenKira23406No ratings yet
- DIAGNOSING HYPERTENSION: BLOOD PRESSURE MEASUREMENT GUIDEDocument37 pagesDIAGNOSING HYPERTENSION: BLOOD PRESSURE MEASUREMENT GUIDEDhira 'Princess Kalonk' AninditaNo ratings yet
- Hipertension Arterial 2018Document5 pagesHipertension Arterial 2018HIilda V. SerranoNo ratings yet
- Asimulatorforoscillometricblood PressuresignalsDocument8 pagesAsimulatorforoscillometricblood PressuresignalsCarlos JuniorNo ratings yet
- NCP - Preeclampsia (A)Document6 pagesNCP - Preeclampsia (A)Ronel ResurricionNo ratings yet
- Measurement of BPDocument6 pagesMeasurement of BPNiko DagunoNo ratings yet
- BP - LippincottDocument7 pagesBP - LippincottForrest LloydNo ratings yet
- BP ChecklistDocument4 pagesBP Checklistkuroko senpaiNo ratings yet
- Screening for Hypertension RiskDocument41 pagesScreening for Hypertension RiskAfpmc NicuNo ratings yet
- A Simulator For Oscillometric Blood-Pressure Signals To Test Automated Noninvasive SphygmomanometersDocument8 pagesA Simulator For Oscillometric Blood-Pressure Signals To Test Automated Noninvasive SphygmomanometerssemiconductormanNo ratings yet
- II HTNDocument34 pagesII HTNJoe TincilNo ratings yet
- Measuring Basic Observations Vital Signs OSCE GuideDocument9 pagesMeasuring Basic Observations Vital Signs OSCE GuidedrpeterimojeNo ratings yet
- Severe TBI 2017Document18 pagesSevere TBI 2017DM internaNo ratings yet
- 2014 Oman Heart Association Guidelines For The Management of HypertensionDocument28 pages2014 Oman Heart Association Guidelines For The Management of Hypertensionمحمداحمد محمدنور ابايزيدNo ratings yet
- Readiness For Enhanced Health ManagementDocument6 pagesReadiness For Enhanced Health ManagementJIMENEZ, TRISHA MARIE D.No ratings yet
- Therapy in Hypertension: Position of Fixed Combination.: Harun Rasyid LubisDocument67 pagesTherapy in Hypertension: Position of Fixed Combination.: Harun Rasyid LubispernandaselpiaNo ratings yet
- Jolly Hannah Management of Hypertensive Emergencies 2021Document7 pagesJolly Hannah Management of Hypertensive Emergencies 2021Angela Moreira ArteagaNo ratings yet
- Course Task CU 7Document7 pagesCourse Task CU 7Kyla PamaNo ratings yet
- Classification Systolic (MM HG) Diastolic (MM HG)Document4 pagesClassification Systolic (MM HG) Diastolic (MM HG)Michelle MartillanoNo ratings yet
- Ambulatory Blood Pressure MonitoringDocument2 pagesAmbulatory Blood Pressure Monitoringapi-658183316No ratings yet
- Essentials of Ambulatory Blood Pressure Monitoring (ABPMDocument7 pagesEssentials of Ambulatory Blood Pressure Monitoring (ABPMApt RiskaNo ratings yet
- Course Task Week 7 NCMB 312Document6 pagesCourse Task Week 7 NCMB 312Angie BaylonNo ratings yet
- Cardio To C OgraphyDocument25 pagesCardio To C OgraphyLhiz Poclan KiwasNo ratings yet
- PDF Nursing Care PlanDocument16 pagesPDF Nursing Care PlanMichael MabiniNo ratings yet
- Urgent and Emergency HypertensionDocument36 pagesUrgent and Emergency HypertensionsrieastutikNo ratings yet
- Ectopic and Abortion NCPDocument6 pagesEctopic and Abortion NCPElizabeth Quiñones100% (1)
- Nursing Care Plan for Mr. Hulu's Fluid Volume DeficitDocument4 pagesNursing Care Plan for Mr. Hulu's Fluid Volume DeficitMariel GamaloNo ratings yet
- 2023 Measure 317 MIPSCQMDocument10 pages2023 Measure 317 MIPSCQMramshaltaf2311No ratings yet
- Hypertension 2020-22: HighlightsDocument15 pagesHypertension 2020-22: HighlightsDuaa ShamiehNo ratings yet
- How To Take The Vital Signs of TheDocument19 pagesHow To Take The Vital Signs of TheDanielle ReginaldoNo ratings yet
- Updated Joint StatementDocument1 pageUpdated Joint StatementSmyle TinipacNo ratings yet
- Diagnostic Pitfall of Hypertension: Dr. Md. Faruk Hossen MCPS, Fcps Consultant (Medicine) Uhc, Adamdighi, BoguraDocument22 pagesDiagnostic Pitfall of Hypertension: Dr. Md. Faruk Hossen MCPS, Fcps Consultant (Medicine) Uhc, Adamdighi, BoguraDr. RajibNo ratings yet
- Diagnosis Treatment of Resistant HypertensionDocument68 pagesDiagnosis Treatment of Resistant HypertensionJacob Alexander MarpaungNo ratings yet
- Assessing Blood PressureDocument4 pagesAssessing Blood PressureCraigyyNo ratings yet
- NCP2Document4 pagesNCP2Aubrey Marie GuerreroNo ratings yet
- Manual Blood Pressure Competency ChecklistDocument1 pageManual Blood Pressure Competency Checklistshubham verma100% (1)
- De Paula 2021Document8 pagesDe Paula 2021TAINAH DE PAULANo ratings yet
- AcneDocument20 pagesAcneAhmed RamiNo ratings yet
- NUGGETS INTERNAL MEDICINE FOR USMLE STEP-2Document75 pagesNUGGETS INTERNAL MEDICINE FOR USMLE STEP-2hippocamperNo ratings yet
- Tiki Taka CK SurgeryDocument50 pagesTiki Taka CK SurgeryEmad MerganNo ratings yet
- Ab Domino PerinealDocument1 pageAb Domino PerinealAhmed RamiNo ratings yet
- Sarw GTDocument1 pageSarw GTAhmed RamiNo ratings yet
- KD 2 Ahqkg N0 LP KHSVGN GDocument1 pageKD 2 Ahqkg N0 LP KHSVGN GAhmed RamiNo ratings yet
- Dermatology MnemonicDocument16 pagesDermatology MnemonicAhmed RamiNo ratings yet
- Making SenseDocument9 pagesMaking SenseAhmed RamiNo ratings yet
- luJVYQb-jW1ImJJ YjWxDocument1 pageluJVYQb-jW1ImJJ YjWxAhmed RamiNo ratings yet
- GIDocument42 pagesGIAhmed RamiNo ratings yet
- 2019 Course CatalogDocument31 pages2019 Course CatalogDeepen SharmaNo ratings yet
- Madeleine Ker - TakeoverDocument91 pagesMadeleine Ker - Takeover66677785100% (1)
- Baseline Program Rev 3A Presentation 25 July 2020Document24 pagesBaseline Program Rev 3A Presentation 25 July 2020Shakti Sourava RautrayaNo ratings yet
- Antonovsky (1979)Document280 pagesAntonovsky (1979)M.Fakhrul Kurnia100% (1)
- CIRC 314-AN 178 INP EN EDENPROD 195309 v1Document34 pagesCIRC 314-AN 178 INP EN EDENPROD 195309 v1xloriki_100% (1)
- Chain Surveying InstrumentsDocument5 pagesChain Surveying InstrumentsSachin RanaNo ratings yet
- Aacra Draft Preliminary Report PDFDocument385 pagesAacra Draft Preliminary Report PDFBeselam SeyedNo ratings yet
- 2 - Soil-Only Landfill CoversDocument13 pages2 - Soil-Only Landfill Covers齐左No ratings yet
- Interpreting Piping and Instrumentation DiagramsDocument41 pagesInterpreting Piping and Instrumentation DiagramsFredric Tun100% (2)
- Telco XPOL MIMO Industrial Class Solid Dish AntennaDocument4 pagesTelco XPOL MIMO Industrial Class Solid Dish AntennaOmar PerezNo ratings yet
- Flowing Gas Material BalanceDocument4 pagesFlowing Gas Material BalanceVladimir PriescuNo ratings yet
- WOOD Investor Presentation 3Q21Document65 pagesWOOD Investor Presentation 3Q21Koko HadiwanaNo ratings yet
- DK Children Nature S Deadliest Creatures Visual Encyclopedia PDFDocument210 pagesDK Children Nature S Deadliest Creatures Visual Encyclopedia PDFThu Hà100% (6)
- Internal Audit ChecklistDocument18 pagesInternal Audit ChecklistAkhilesh Kumar75% (4)
- Elevator Traction Machine CatalogDocument24 pagesElevator Traction Machine CatalogRafif100% (1)
- 07 Raction KineticsDocument43 pages07 Raction KineticsestefanoveiraNo ratings yet
- Detection and Attribution Methodologies Overview: Appendix CDocument9 pagesDetection and Attribution Methodologies Overview: Appendix CDinesh GaikwadNo ratings yet
- Feline DermatologyDocument55 pagesFeline DermatologySilviuNo ratings yet
- Metal Framing SystemDocument56 pagesMetal Framing SystemNal MénNo ratings yet
- HSC 405 Grant ProposalDocument23 pagesHSC 405 Grant Proposalapi-355220460100% (2)
- Sto - Cristo Proper Integrated School 1 Grading Grade 9 Science Table of SpecializationDocument2 pagesSto - Cristo Proper Integrated School 1 Grading Grade 9 Science Table of Specializationinah jessica valerianoNo ratings yet
- NDE Procedure - Radiographic TestingDocument43 pagesNDE Procedure - Radiographic TestingJeganeswaranNo ratings yet
- Handout Tematik MukhidDocument72 pagesHandout Tematik MukhidJaya ExpressNo ratings yet
- Henry Stevens - Hitler's Flying Saucers - A Guide To German Flying Discs of The Second World War New Edition (2013, Adventures Unlimited Press) - Libgen - lc-116-120Document5 pagesHenry Stevens - Hitler's Flying Saucers - A Guide To German Flying Discs of The Second World War New Edition (2013, Adventures Unlimited Press) - Libgen - lc-116-120sejoh34456No ratings yet
- CP 343-1Document23 pagesCP 343-1Yahya AdamNo ratings yet
- Project On Stones & TilesDocument41 pagesProject On Stones & TilesMegha GolaNo ratings yet
- Religion in Space Science FictionDocument23 pagesReligion in Space Science FictionjasonbattNo ratings yet
- Private Schools Provide Better EducationDocument2 pagesPrivate Schools Provide Better EducationcitraNo ratings yet
- CAT Ground Engaging ToolsDocument35 pagesCAT Ground Engaging ToolsJimmy Nuñez VarasNo ratings yet