You might also like
- Pharmacogenomics: From Discovery to Clinical ImplementationFrom EverandPharmacogenomics: From Discovery to Clinical ImplementationShowkat Ahmad GanieNo ratings yet
- Farmakoterapi - TuberkulosisDocument92 pagesFarmakoterapi - TuberkulosisMario MooreNo ratings yet
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisFrom EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisRating: 3.5 out of 5 stars3.5/5 (2)
- Seminar ISTC TB Feb 2016Document12 pagesSeminar ISTC TB Feb 2016christine nathalia loupattyNo ratings yet
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- Asthma + COPD - 2022 LectureDocument85 pagesAsthma + COPD - 2022 Lecturedesti purnama sariNo ratings yet
- Gasem MH HANTA Salatiga 2019Document43 pagesGasem MH HANTA Salatiga 2019ChristianNo ratings yet
- Baca Dari PapdiDocument4 pagesBaca Dari PapdiAriane BeninaNo ratings yet
- TiroidDocument26 pagesTiroidJoni Riana MustaqimNo ratings yet
- Infeksi Virus Dengue: Demam Berdarah Dengue Demam DengueDocument62 pagesInfeksi Virus Dengue: Demam Berdarah Dengue Demam DengueMarwi VinaNo ratings yet
- FluDocument31 pagesFluSheril Sularte CasanesNo ratings yet
- Therapeutically Administered Ribonucleoside Analogue Mk-4482/Eidd-2801 Blocks Sars-Cov-2 Transmission in FerretsDocument15 pagesTherapeutically Administered Ribonucleoside Analogue Mk-4482/Eidd-2801 Blocks Sars-Cov-2 Transmission in FerretsCarlosgustavo SaavedrarubioNo ratings yet
- 2.tukak PeptikDocument42 pages2.tukak PeptikEfvi VhyLiaNo ratings yet
- TB Milier PrintDocument15 pagesTB Milier PrintgigibesiNo ratings yet
- Hepatopulmonary Syndrome (2014)Document47 pagesHepatopulmonary Syndrome (2014)Robert G. Gish, MDNo ratings yet
- Daftar Pustaka Hipertensi Pada Usia MudaDocument10 pagesDaftar Pustaka Hipertensi Pada Usia MudaToby Hadinata WiranegaraNo ratings yet
- Advance Care Planning English VersionDocument9 pagesAdvance Care Planning English VersionAlma NurfitriaNo ratings yet
- PansitopeniaDocument33 pagesPansitopeniaBrad WrightNo ratings yet
- TB Paru FK UncenDocument66 pagesTB Paru FK UncenAndira Trianingrum TukanNo ratings yet
- Hipertensi: Tekanan Darah TinggiDocument33 pagesHipertensi: Tekanan Darah TinggiErika SetyodiharjoNo ratings yet
- CR DR - Dedi Hidropneumothorax Ec TB ParuDocument38 pagesCR DR - Dedi Hidropneumothorax Ec TB ParuBunga Listia ParamitaNo ratings yet
- Hipertensi JNC 8Document7 pagesHipertensi JNC 8Elisse StephanieNo ratings yet
- Acs OsceDocument4 pagesAcs OsceYohanes ArviNo ratings yet
- Terapi OksigenDocument33 pagesTerapi OksigenMirzaNo ratings yet
- Congenital Tuberculosis A Review ArticleDocument5 pagesCongenital Tuberculosis A Review ArticleMasita RochsalehaNo ratings yet
- TB FixDocument11 pagesTB FixDevina SagitaniaNo ratings yet
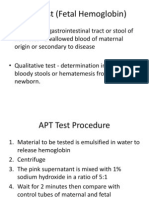
- APT Test (Fetal Hemoglobin)Document11 pagesAPT Test (Fetal Hemoglobin)Diovic TanNo ratings yet
- Manifestasi Klinis Dan Penanganan Demam Berdarah Dengue Grade 1: Sebuah Tinjauan PustakaDocument5 pagesManifestasi Klinis Dan Penanganan Demam Berdarah Dengue Grade 1: Sebuah Tinjauan Pustakanur aisyahNo ratings yet
- Sepsis and Septic Shock GuidelinesfinalDocument51 pagesSepsis and Septic Shock GuidelinesfinalElteyb Nor eldaimNo ratings yet
- LEaflet TBCDocument3 pagesLEaflet TBCatik mayasariNo ratings yet
- G IN A: Lobal Itiative For SthmaDocument66 pagesG IN A: Lobal Itiative For SthmaNerissaArvianaShintaraNo ratings yet
- Perioperative Management in Diabetes MellitusDocument20 pagesPerioperative Management in Diabetes MellitusChristopher RyalinoNo ratings yet
- Istc 2014Document67 pagesIstc 2014Rosy KusumaNo ratings yet
- 2 DHF InternaDocument59 pages2 DHF Internasaladass 2No ratings yet
- COPD - Update Diagnosis and Management of Stable COPDDocument29 pagesCOPD - Update Diagnosis and Management of Stable COPDIwanNo ratings yet
- Kul Sem 4 Heat Stroke N Fever UHT 2016Document63 pagesKul Sem 4 Heat Stroke N Fever UHT 2016NandaSuryaWijayaNo ratings yet
- TB-DM: International Standards For Tuberculosis Care 3 EdDocument36 pagesTB-DM: International Standards For Tuberculosis Care 3 EdDWI RATNA100% (1)
- Interpretation of Histograms and Its Correlation WDocument5 pagesInterpretation of Histograms and Its Correlation WrezqiNo ratings yet
- Antimicrobial Stewardship ProgrammeDocument12 pagesAntimicrobial Stewardship ProgrammeDesmiyati AdoeNo ratings yet
- Geriatric Medicine KuliahDocument38 pagesGeriatric Medicine KuliahLia pramitaNo ratings yet
- Bilas LambungDocument12 pagesBilas LambungNthie UnguNo ratings yet
- PneumothoraxDocument14 pagesPneumothoraxAsterlita WenasNo ratings yet
- Jurnal AMS PDFDocument8 pagesJurnal AMS PDFputriseptinaNo ratings yet
- Data - anggotaKABUPATEN SIJUNJUNG-1Document8 pagesData - anggotaKABUPATEN SIJUNJUNG-1deviya srimarlisNo ratings yet
- Penatalaksanaan IRISDocument39 pagesPenatalaksanaan IRISdian sudianaNo ratings yet
- Journal Reading OrthopaedicsDocument9 pagesJournal Reading OrthopaedicsRizka Nurul FirdausNo ratings yet
- Intrapleural Ruptured Hydatid Cyst of Liver Presented As Eosinophilic Pleural Effusion: Case ReportDocument7 pagesIntrapleural Ruptured Hydatid Cyst of Liver Presented As Eosinophilic Pleural Effusion: Case ReportIJAR JOURNALNo ratings yet
- Final Assignment of Big Data in Hospital Wendry Pasorong MHM Batch 3 UphDocument11 pagesFinal Assignment of Big Data in Hospital Wendry Pasorong MHM Batch 3 UphwendryNo ratings yet
- Radiologi ILO Terbaru (PIPKRA 2011)Document47 pagesRadiologi ILO Terbaru (PIPKRA 2011)elsaNo ratings yet
- Bahan Kuliah HIV-AIDSDocument17 pagesBahan Kuliah HIV-AIDSKiki Rizky Andani NasutionNo ratings yet
- Diabetes Mellitus: DR Hiew Fu LiongDocument30 pagesDiabetes Mellitus: DR Hiew Fu LiongamminsaffriNo ratings yet
- Chapter 193:: Herpes Simplex:: Adriana R. Marques & Jeffrey I. CohenDocument16 pagesChapter 193:: Herpes Simplex:: Adriana R. Marques & Jeffrey I. CohenwadejackNo ratings yet
- Case Report Tifoid FeverDocument37 pagesCase Report Tifoid FeverAmi ArniamanthaNo ratings yet
- ICD 10 Codes For HIVDocument2 pagesICD 10 Codes For HIVmahi50No ratings yet
- PhysioEx Exercise 4 Activity 2Document3 pagesPhysioEx Exercise 4 Activity 2PatriNo ratings yet
- The Brief Case Incidental Finding of Cystic Echinococcosis During Evaluation For HaematemesisDocument3 pagesThe Brief Case Incidental Finding of Cystic Echinococcosis During Evaluation For HaematemesisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Aspek Laboratorium Kelainan Hormon Tiroid Dan Paratiroid 2016Document52 pagesAspek Laboratorium Kelainan Hormon Tiroid Dan Paratiroid 2016Teguh Amin SunyotoNo ratings yet
- Acute Gastroenteritis in Adult: DR - Umar Zein, SPPD, Mha, DTMH, KptiDocument30 pagesAcute Gastroenteritis in Adult: DR - Umar Zein, SPPD, Mha, DTMH, KptiSarachanda SallyNo ratings yet
- Hubungan Antara TB Dan HIVDocument52 pagesHubungan Antara TB Dan HIVNurlaela Eka RostariNo ratings yet
- 3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualDocument28 pages3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualjimmyneumologiaNo ratings yet
- Handbook ENGLISH FOR PHARMACY IIDocument37 pagesHandbook ENGLISH FOR PHARMACY IIAjeng Afriliana75% (4)
- Molecules - 1 (Carbs & Lipids) V2Document13 pagesMolecules - 1 (Carbs & Lipids) V2ormattNo ratings yet
- Antibiotics, Misuse and ConsequencesDocument67 pagesAntibiotics, Misuse and Consequencestummalapalli venkateswara raoNo ratings yet
- Chi Cards 1Document43 pagesChi Cards 1SwordAceNo ratings yet
- Hazard Identification and Risk AssesmentDocument4 pagesHazard Identification and Risk AssesmentsuyatnofkmundipNo ratings yet
- Case Presentation OF: Iron Deficiency AnemiaDocument33 pagesCase Presentation OF: Iron Deficiency Anemiaitshurt_teardrops100% (1)
- 2) Incaaam PP ThreadliftDocument47 pages2) Incaaam PP ThreadliftFitri Fratiwi100% (4)
- Background: Abruptio PlacentaeDocument6 pagesBackground: Abruptio PlacentaeEj ZGNo ratings yet
- Sterilization of Water Using Bleaching PowderDocument15 pagesSterilization of Water Using Bleaching PowderSupriyaNo ratings yet
- MSDS ThievesDocument11 pagesMSDS ThievesATOMY KESEHATANNo ratings yet
- Filipino Scientists: GE 07 Science, Technology and SocietyDocument4 pagesFilipino Scientists: GE 07 Science, Technology and SocietyEvangeline EnocNo ratings yet
- EsophagogastroduodenosDocument34 pagesEsophagogastroduodenosAngela Beatriz Dela Vega100% (1)
- Essay ModelDocument4 pagesEssay ModelEmma MalekNo ratings yet
- The Secrets of Hunza WaterDocument3 pagesThe Secrets of Hunza Wateresmeille100% (2)
- Gul Ahmed 1Document4 pagesGul Ahmed 1SALMAN SHAKEELNo ratings yet
- Cell LineageDocument7 pagesCell LineageAmar Kant JhaNo ratings yet
- History of Nursing and The Development of The ProfessionDocument4 pagesHistory of Nursing and The Development of The Professionastraia celesteNo ratings yet
- Nguyen 2019Document6 pagesNguyen 2019ClintonNo ratings yet
- Parasite 1Document22 pagesParasite 1OnSolomonNo ratings yet
- Overview of Stroke - Knowledge at AMBOSSDocument19 pagesOverview of Stroke - Knowledge at AMBOSSandimija16No ratings yet
- Antifertility DrugsDocument12 pagesAntifertility DrugsforplancessNo ratings yet
- Patient'S Case Performa FileDocument13 pagesPatient'S Case Performa Filevipul tandonNo ratings yet
- Minamata Mercury Diseases (Presentation)Document34 pagesMinamata Mercury Diseases (Presentation)thanes_kumar100% (4)
- Diabetes MelitusDocument44 pagesDiabetes MelitusDwi Novianti SugihartiNo ratings yet
- BorneoDocument1 pageBorneoapi-235669157No ratings yet
- MSDS Jun-Air SJ-27FDocument8 pagesMSDS Jun-Air SJ-27FJuan Eduardo LoayzaNo ratings yet
- Cotton Varieties HybridsDocument15 pagesCotton Varieties HybridsAjay KumarNo ratings yet
- Non-Mendelian Inheritance2Document41 pagesNon-Mendelian Inheritance2Jeremy Christian MendozaNo ratings yet
- 1.-Write The Verb in Brackets in Past Simple or Present PerfectDocument1 page1.-Write The Verb in Brackets in Past Simple or Present PerfectLaura LNo ratings yet
- BourkeDocument8 pagesBourkeMilan BursacNo ratings yet