You might also like
- CVAD For NursesDocument54 pagesCVAD For NursesRitaLakhaniNo ratings yet
- DialysisDocument20 pagesDialysisSiwani rai100% (1)
- Central Venous CatheterizationDocument34 pagesCentral Venous CatheterizationMujeeb NangrajNo ratings yet
- IV TherapyDocument39 pagesIV TherapyChannelGNo ratings yet
- Procedure-Central Venous Access Catheter InsertionDocument18 pagesProcedure-Central Venous Access Catheter Insertionmohamad dildarNo ratings yet
- Care of CVCDocument32 pagesCare of CVCholyfamily100% (1)
- Peripheral Intravenous Cannulation PolicyDocument14 pagesPeripheral Intravenous Cannulation PolicyRoksana AkhterNo ratings yet
- ICU Accomplishment Report and Improvement PlanDocument5 pagesICU Accomplishment Report and Improvement PlanMikhaelEarlSantosTacordaNo ratings yet
- Pulmonary EmbolismDocument19 pagesPulmonary EmbolismIbrahimNo ratings yet
- Adam Low - CLABSI Best Practice and BundlesDocument34 pagesAdam Low - CLABSI Best Practice and Bundlesvera indrawatiNo ratings yet
- Approach To Septic ShockDocument16 pagesApproach To Septic ShockRaja EllysyaNo ratings yet
- Hyphema 2Document7 pagesHyphema 2heidyNo ratings yet
- Securing Airways and Suctioning Endotracheal TubesDocument28 pagesSecuring Airways and Suctioning Endotracheal TubesJohn Mark ParacadNo ratings yet
- Central Line Associated Bloodstream Infections (CLABSI)Document41 pagesCentral Line Associated Bloodstream Infections (CLABSI)roslah sopiah100% (1)
- 2714 - Peripheral Venous Catheter Care Policy For AdultsDocument10 pages2714 - Peripheral Venous Catheter Care Policy For AdultssofiinhaptNo ratings yet
- Management of Febrile NeutropaeniaDocument8 pagesManagement of Febrile NeutropaeniagigibesiNo ratings yet
- Etat + PDFDocument56 pagesEtat + PDFShandy BNo ratings yet
- Assisting Central Venous Catheter (CVC) Insertion (Procedure1)Document7 pagesAssisting Central Venous Catheter (CVC) Insertion (Procedure1)BsBs A7medNo ratings yet
- Cardiac Testing Role Risk Stratifying ED Chest PainDocument17 pagesCardiac Testing Role Risk Stratifying ED Chest PainGiorgiana pNo ratings yet
- Clinical Aspects of NeoplasiaDocument23 pagesClinical Aspects of NeoplasiaJahanzaib BashirNo ratings yet
- E Learning Geriatric Oncology An IntroductionDocument65 pagesE Learning Geriatric Oncology An IntroductionHarold JeffersonNo ratings yet
- Knowledge and Practice Towards Care and MaintenancDocument7 pagesKnowledge and Practice Towards Care and MaintenancyunishaNo ratings yet
- Status Asthmaticus!!!!!! PDFDocument13 pagesStatus Asthmaticus!!!!!! PDFKassandra Mildred GutierrezNo ratings yet
- Hemodiafiltration Kuhlmann PDFDocument31 pagesHemodiafiltration Kuhlmann PDFDavid SantosoNo ratings yet
- Kidney TransplantDocument11 pagesKidney TransplantPrincess Xzmae RamirezNo ratings yet
- CNS Congenital AnomaliesDocument74 pagesCNS Congenital AnomaliesMoh DrhusseinyNo ratings yet
- 13.24 Abdominal-InjuryDocument42 pages13.24 Abdominal-InjuryMuhammad FajarNo ratings yet
- Antimicrobialstewardship Approachesinthe Intensivecareunit: Sarah B. Doernberg,, Henry F. ChambersDocument22 pagesAntimicrobialstewardship Approachesinthe Intensivecareunit: Sarah B. Doernberg,, Henry F. ChambersecaicedoNo ratings yet
- Central LinesDocument19 pagesCentral LinesJosef TrapaniNo ratings yet
- 3rd Year Pathology Study GuideDocument67 pages3rd Year Pathology Study Guideঔৣ࿐࿐࿐irsнαd кнαท࿐࿐࿐ঔৣ BurkiNo ratings yet
- Objectives: General Objective: Specific ObjectivesDocument8 pagesObjectives: General Objective: Specific ObjectivesLora CarpioNo ratings yet
- Septic Shock Treatment & ManagementDocument18 pagesSeptic Shock Treatment & ManagementDiego ErazoNo ratings yet
- Oxygen Therapy: by DR Finny Theo, MBBS, (DNB)Document59 pagesOxygen Therapy: by DR Finny Theo, MBBS, (DNB)The Telugu DoctorNo ratings yet
- Lumbar PunctureDocument37 pagesLumbar PunctureRahul Varshney100% (1)
- Fluid Management - Presentation PDFDocument16 pagesFluid Management - Presentation PDFjuniorebinda100% (1)
- Siobhan K Smith Nursing StudentDocument2 pagesSiobhan K Smith Nursing Studentapi-456190363No ratings yet
- Informed ConsentDocument25 pagesInformed ConsentMaylodie ingallaNo ratings yet
- 050 PPT - RetinoblastomaDocument61 pages050 PPT - RetinoblastomaAnastasia TjanNo ratings yet
- Lung Abscess Symptoms, Causes and TreatmentDocument40 pagesLung Abscess Symptoms, Causes and Treatmentghhh100% (1)
- Week 4 Ethics Decision MakingDocument59 pagesWeek 4 Ethics Decision Makingmaha abdallahNo ratings yet
- ICU TriageDocument27 pagesICU TriageAkmal FahrezzyNo ratings yet
- Airway Obstruction - Types, Causes, and SymptomsDocument6 pagesAirway Obstruction - Types, Causes, and SymptomsGilbertLiem100% (1)
- Neuroblastoma: A Cancer of the Sympathetic Nervous SystemDocument153 pagesNeuroblastoma: A Cancer of the Sympathetic Nervous SystemWael ElsawyNo ratings yet
- Fulminant Hepatic FailureDocument12 pagesFulminant Hepatic Failureafghansyah arfiantoNo ratings yet
- Hospital Infection Control Manual AIIMS Raipur2019 (Word)Document204 pagesHospital Infection Control Manual AIIMS Raipur2019 (Word)Dipali SolankiNo ratings yet
- HydroceleDocument11 pagesHydroceleagungsh100% (1)
- Name: Muhyee S. Idjad Year&Sec: BSNIII-B: What Is in A Emergency Cart?Document3 pagesName: Muhyee S. Idjad Year&Sec: BSNIII-B: What Is in A Emergency Cart?Yeng Cries50% (2)
- Management of Vacuum Assisted Closure TherapyDocument14 pagesManagement of Vacuum Assisted Closure TherapyVoiculescu MihaelaNo ratings yet
- Urinary Retention PostpartumDocument5 pagesUrinary Retention PostpartumpaswordnyalupaNo ratings yet
- TRIAGE POLICIES JuvyDocument6 pagesTRIAGE POLICIES JuvyCuyapo Infirmary Lying-In HospitalNo ratings yet
- Bone Marrow ChecklistDocument2 pagesBone Marrow ChecklistHasyim SuparlanNo ratings yet
- AppendicitisDocument36 pagesAppendicitisPetro MyronovNo ratings yet
- BlepharitisDocument20 pagesBlepharitisNorshahidah IedaNo ratings yet
- Brain AbscessDocument25 pagesBrain AbscessprembarnabasNo ratings yet
- Cronic WoundsDocument11 pagesCronic WoundsAyline Araceli AlavaNo ratings yet
- BurnDocument69 pagesBurnntandayuNo ratings yet
- Disturbances in Respiratory FunctionDocument6 pagesDisturbances in Respiratory FunctionSeff CausapinNo ratings yet
- Spinal TuberculosisDocument46 pagesSpinal TuberculosisAbby Austero100% (1)
- 01 Admission Discharge Criteria and TriageDocument5 pages01 Admission Discharge Criteria and TriageSuhasani JainNo ratings yet
- Dr. Jerry PDFDocument8 pagesDr. Jerry PDFFlorence LiemNo ratings yet
- Antihemophilic Factor (Human) : Ko atew-DVIDocument4 pagesAntihemophilic Factor (Human) : Ko atew-DVIFlorence LiemNo ratings yet
- Overview of Mechanical Ventilation Settings, Modes, TroubleshootingDocument24 pagesOverview of Mechanical Ventilation Settings, Modes, TroubleshootingRochim CoolNo ratings yet
- PancreatitisDocument7 pagesPancreatitisFlorence LiemNo ratings yet
- ESPEN Guidelines On Enteral Nutrition - Liver Disease PDFDocument10 pagesESPEN Guidelines On Enteral Nutrition - Liver Disease PDFFlorence LiemNo ratings yet
- HE EASL2013 Update Newsletter (Albumin) PDFDocument10 pagesHE EASL2013 Update Newsletter (Albumin) PDFFlorence LiemNo ratings yet
- Hepatic Encephalopathy Therapy - An Overview, 2010 PDFDocument10 pagesHepatic Encephalopathy Therapy - An Overview, 2010 PDFFlorence LiemNo ratings yet
- Bdb06ff135c7ccb File 2Document29 pagesBdb06ff135c7ccb File 2Mary ThaherNo ratings yet
- EASL Meeting HE PDFDocument16 pagesEASL Meeting HE PDFFlorence LiemNo ratings yet
- Minophagen PDFDocument6 pagesMinophagen PDFFlorence LiemNo ratings yet
- Cholangio CarcinomaDocument22 pagesCholangio CarcinomaFlorence LiemNo ratings yet
- Hepatitis C APASLfghDocument27 pagesHepatitis C APASLfghAndi BintangNo ratings yet
- Coinfection Hiv Viral Hep PDFDocument42 pagesCoinfection Hiv Viral Hep PDFFlorence LiemNo ratings yet
- Dr. Jerry PDFDocument6 pagesDr. Jerry PDFFlorence LiemNo ratings yet
- L-Ornithine-L-Aspartate Infusion Efficacy in Hepatic Encephalopathy, 2008Document4 pagesL-Ornithine-L-Aspartate Infusion Efficacy in Hepatic Encephalopathy, 2008Florence LiemNo ratings yet
- Dr. Jerry PDFDocument18 pagesDr. Jerry PDFFlorence LiemNo ratings yet
- onlineLibraryTPS - TerbaruDocument10 pagesonlineLibraryTPS - TerbaruFlorence LiemNo ratings yet
- Diagnosis Protocol For DiabetesDocument1 pageDiagnosis Protocol For DiabetesFlorence LiemNo ratings yet
- Glycyrrhizin - A ReviewDocument3 pagesGlycyrrhizin - A ReviewFlorence LiemNo ratings yet
- Therapeutic Efficacy of L-Ornithine-L-Aspartate Infusions in Patients With Cirrhosis and Hepatic Encephalopathy - Results of A Placebo-Controlled, Double-Blind Study, 1997Document10 pagesTherapeutic Efficacy of L-Ornithine-L-Aspartate Infusions in Patients With Cirrhosis and Hepatic Encephalopathy - Results of A Placebo-Controlled, Double-Blind Study, 1997Florence LiemNo ratings yet
- Hepatic Encephalopathy Therapy - An Overview, 2010 PDFDocument10 pagesHepatic Encephalopathy Therapy - An Overview, 2010 PDFFlorence LiemNo ratings yet
- Hepatic Encephalopathy - Suspect It Early in Patients With Cirrhosis, 2011Document9 pagesHepatic Encephalopathy - Suspect It Early in Patients With Cirrhosis, 2011Florence LiemNo ratings yet
- A Systematic Review and Meta-Analysis of The Use Zinc in The Treatment of Hepatic Encephalopathy, 2013Document6 pagesA Systematic Review and Meta-Analysis of The Use Zinc in The Treatment of Hepatic Encephalopathy, 2013Florence LiemNo ratings yet
- Causes of Leukocoria - Retinoblastoma, Cataract, ROP and MoreDocument37 pagesCauses of Leukocoria - Retinoblastoma, Cataract, ROP and MoreAnonymous mFKwUNNo ratings yet
- Graves' Disease Graves 'PenyakitDocument43 pagesGraves' Disease Graves 'PenyakitFlorence LiemNo ratings yet
- Step 2 CK NotesDocument76 pagesStep 2 CK Noteskeyurb100% (1)
- Lecture Chapter 1 PDFDocument30 pagesLecture Chapter 1 PDFmresearchNo ratings yet
- Diacon-P en DT Rev01 0821501 Rev01Document12 pagesDiacon-P en DT Rev01 0821501 Rev01vijayramaswamyNo ratings yet
- Oral Potentially Malignant Lesions GuideDocument9 pagesOral Potentially Malignant Lesions GuideAbd RahmanNo ratings yet
- KSPM 12 02 121Document8 pagesKSPM 12 02 121kang soon cheolNo ratings yet
- Formulation and Evaluation of Wood Apple Supplemented KalakandDocument3 pagesFormulation and Evaluation of Wood Apple Supplemented KalakandDr-Prafull Pratap Singh YadavNo ratings yet
- HEART Grade 9Document3 pagesHEART Grade 9Hansel MusimaNo ratings yet
- Adolescent Medicine PDFDocument292 pagesAdolescent Medicine PDFpblsvraman100% (1)
- HipoglikemiaDocument13 pagesHipoglikemiaRC Ria Chairul100% (1)
- Formulation and Evaluation of Floating Tablet of LevofloxacinDocument8 pagesFormulation and Evaluation of Floating Tablet of LevofloxacinPharma Research LibraryNo ratings yet
- Takra Dhara: Buttermilk Shirodhara ProcedureDocument2 pagesTakra Dhara: Buttermilk Shirodhara ProcedureSwagath NNo ratings yet
- How To Prescribe Drug For DentistsDocument22 pagesHow To Prescribe Drug For DentistsahmedNo ratings yet
- Febrile SeizureDocument16 pagesFebrile SeizureRashed Shatnawi100% (1)
- Approach To The Adult With Anemia - UpToDate PDFDocument66 pagesApproach To The Adult With Anemia - UpToDate PDFJuliana Salerno100% (1)
- BSN ScheduleDocument5 pagesBSN ScheduleKaren LuzonNo ratings yet
- Orthopedics 2 Test NotesDocument6 pagesOrthopedics 2 Test Notesbjpalmer100% (1)
- Mental Health Case Study AssignmentDocument2 pagesMental Health Case Study Assignmentapi-364232905No ratings yet
- PM Journal1Document10 pagesPM Journal1gireesh_babuNo ratings yet
- Shutter Island ReacDocument4 pagesShutter Island ReacBethany CorpuzNo ratings yet
- First Aid and Disease TransmissionDocument5 pagesFirst Aid and Disease TransmissionneopriyanshNo ratings yet
- Daftar Lasa N High Alert PKM SambasDocument5 pagesDaftar Lasa N High Alert PKM SambasROBERTNo ratings yet
- CP Intestinal Obstruction Bibliography VitaeDocument5 pagesCP Intestinal Obstruction Bibliography VitaeKatherine 'Chingboo' Leonico LaudNo ratings yet
- Biomechanical Evaluation of A Second Generation Headless Compression Screw For Ankle Arthrodesis in A Cadaver ModelDocument6 pagesBiomechanical Evaluation of A Second Generation Headless Compression Screw For Ankle Arthrodesis in A Cadaver ModelEMNo ratings yet
- Harga ObatDocument21 pagesHarga ObatRizamdhani AptNo ratings yet
- Comparative Study - Art sr-3Document20 pagesComparative Study - Art sr-3api-3512015400% (1)
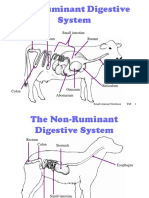
- Ruminant Digestive System ExplainedDocument10 pagesRuminant Digestive System ExplainedshivendraNo ratings yet
- The Twelve Tendino-Muscular Meridians. Part 1Document10 pagesThe Twelve Tendino-Muscular Meridians. Part 1Liew Yetmeng100% (1)
- Madrasah Tsanawiyah (MTS) B: Pondok Pesantren Nurul Yaqin Tanjung Atap AkreditasiDocument3 pagesMadrasah Tsanawiyah (MTS) B: Pondok Pesantren Nurul Yaqin Tanjung Atap AkreditasiAbdur Rahman AwwabienNo ratings yet
- Academic Window BIOLOGY 7 PDFDocument15 pagesAcademic Window BIOLOGY 7 PDFsidharth balaji sridharanNo ratings yet
- MSDS Mu-200Document2 pagesMSDS Mu-200Goldwin Ricky Aritonang87% (15)