You might also like
- Glaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913From EverandGlaucoma A Symposium Presented at a Meeting of the Chicago Ophthalmological Society, November 17, 1913No ratings yet
- Visual Fields Interpretation in Glaucoma A Focus On Static Automated PerimetryDocument8 pagesVisual Fields Interpretation in Glaucoma A Focus On Static Automated PerimetryMoisés Sergio Nina BaldeónNo ratings yet
- Visual Acuity ExaminationDocument46 pagesVisual Acuity ExaminationGepengCungkringNo ratings yet
- A Practical Approach To The Analysis of Visual Field DefectsDocument43 pagesA Practical Approach To The Analysis of Visual Field DefectsstolfishNo ratings yet
- Shyam 2 - ExophthalomometryDocument43 pagesShyam 2 - Exophthalomometrykshitij Shivhare100% (1)
- Electronic Commerce: Electronic Commerce, Commonly Known As E-Commerce, Ecommerce, Ecommerce or E-Comm, RefersDocument3 pagesElectronic Commerce: Electronic Commerce, Commonly Known As E-Commerce, Ecommerce, Ecommerce or E-Comm, RefersSahil Gupta100% (1)
- Goldmann Perimeter 940 ManualDocument19 pagesGoldmann Perimeter 940 ManualPablo Corona100% (1)
- EUPO2013 Coursebook OnlineDocument220 pagesEUPO2013 Coursebook Onlineiuliad88100% (1)
- 09 LensDocument37 pages09 LensFrederica Mutiara100% (1)
- 936Document4 pages936ElBuen JohnNo ratings yet
- Essentials in Ophthalmology Glaucoma: F. Grehn R. Stamper EditorsDocument195 pagesEssentials in Ophthalmology Glaucoma: F. Grehn R. Stamper EditorsBianca AdelinaNo ratings yet
- Red EyeDocument45 pagesRed EyeDavidVictoriousLukas100% (1)
- CH 2 - Binocular Vision and Space Perception, p.7-37Document31 pagesCH 2 - Binocular Vision and Space Perception, p.7-37Enrique AgurtoNo ratings yet
- Esodeviation الحول الإنسيDocument33 pagesEsodeviation الحول الإنسيYaman MuhaisenNo ratings yet
- EGurukul - RetinaDocument23 pagesEGurukul - RetinaOscar Daniel Mendez100% (1)
- The Optical Quality of The CorneaDocument32 pagesThe Optical Quality of The CorneaacalossiNo ratings yet
- AnisometropiaDocument16 pagesAnisometropiadilip100% (1)
- Lensometer & Lens Clock/Gauge: Man Mohan Shah M.Optom 1 YrDocument53 pagesLensometer & Lens Clock/Gauge: Man Mohan Shah M.Optom 1 YrManmohan Shah100% (1)
- Grading ScaleDocument2 pagesGrading ScaleFelipe SanchezNo ratings yet
- Pupillary DisorderDocument19 pagesPupillary DisorderWan HafizNo ratings yet
- Glaucoma and Ocular HypertensionDocument6 pagesGlaucoma and Ocular HypertensionsoniasistNo ratings yet
- (K14) - Contact LensesDocument33 pages(K14) - Contact LensesSyarifah FauziahNo ratings yet
- Eye LidDocument36 pagesEye Lidعبدالسلام ميلاد درباشNo ratings yet
- Clinical Study On Scleral Lenses by Dr. Elise KramerDocument8 pagesClinical Study On Scleral Lenses by Dr. Elise KramerMiami Contact Lens InstituteNo ratings yet
- Retinitis PigmentosaDocument35 pagesRetinitis Pigmentosawessam284No ratings yet
- Refractive Errors: Dr. Kemal DikiciDocument77 pagesRefractive Errors: Dr. Kemal DikiciFirman CappoNo ratings yet
- UveaDocument83 pagesUveaShewit TeklehaymanotNo ratings yet
- Artificial EyeDocument24 pagesArtificial Eyeapoorva1509No ratings yet
- 1 - Orientation, History Taking and ExaminationDocument96 pages1 - Orientation, History Taking and ExaminationHari ShresthaNo ratings yet
- Dr. Mamta Dept of Ophthalmology RNT Medical College, UdaipurDocument56 pagesDr. Mamta Dept of Ophthalmology RNT Medical College, UdaipurGideon IrwandaNo ratings yet
- #The EyelidDocument7 pages#The Eyelidameerabest100% (1)
- Night MiopiaDocument8 pagesNight MiopiamurilobsouzaNo ratings yet
- Clinical Skills Week 1Document3 pagesClinical Skills Week 1Aishah SiddiqahNo ratings yet
- Myopia ManualDocument337 pagesMyopia ManualRealPurgatory100% (1)
- Understanding Visual Fields Part I Goldmann PerimeDocument11 pagesUnderstanding Visual Fields Part I Goldmann PerimeAngelaNo ratings yet
- 19 Rationale of Retinal Detachment ManagementDocument87 pages19 Rationale of Retinal Detachment ManagementvajasaNo ratings yet
- Basic AberrometryDocument54 pagesBasic Aberrometrysightbd100% (2)
- WIP January February 2013Document52 pagesWIP January February 2013Orlando BarriosNo ratings yet
- GoniosDocument55 pagesGoniosdrquan100% (1)
- 06 Refractive ErrorDocument12 pages06 Refractive ErrorMwanja MosesNo ratings yet
- Soflex ND Fitting Guide-Moodi-OphtalmicDocument49 pagesSoflex ND Fitting Guide-Moodi-OphtalmicAndreea Cristea100% (1)
- Kelainan RefraksiDocument39 pagesKelainan RefraksiAlvin PratamaNo ratings yet
- Optics and Refraction For 5 Year Medical Students Mutaz Gharaibeh, MDDocument52 pagesOptics and Refraction For 5 Year Medical Students Mutaz Gharaibeh, MDHidayadNo ratings yet
- Refraction and AccommodationDocument80 pagesRefraction and Accommodationapi-19916399100% (2)
- Optics and Refraction For 5 Year Medical Students Mutaz Gharaibeh, MDDocument52 pagesOptics and Refraction For 5 Year Medical Students Mutaz Gharaibeh, MDShahar ShababNo ratings yet
- Physiology of Optic-VioDocument42 pagesPhysiology of Optic-VioViora RiandaNo ratings yet
- Ophtha - Eor and LensDocument86 pagesOphtha - Eor and Lensapi-3856051No ratings yet
- 3 - Refractive ErrorsDocument17 pages3 - Refractive ErrorsF ParikhNo ratings yet
- Refractive ErrorsDocument38 pagesRefractive ErrorszahraaNo ratings yet
- Anisometropia 4Document18 pagesAnisometropia 4Mamtha MMNo ratings yet
- Refraction Error VinaDocument27 pagesRefraction Error VinaHardiNo ratings yet
- Accomodation and Its Anomalies KyxDocument35 pagesAccomodation and Its Anomalies KyxCharles AntonyNo ratings yet
- Refraction 2Document47 pagesRefraction 2RuDy RaviNo ratings yet
- Refraction Error: Alvina Elsa BidariDocument25 pagesRefraction Error: Alvina Elsa BidariBayu AdityaNo ratings yet
- TBL 1 - Refractive Error SlidesDocument66 pagesTBL 1 - Refractive Error SlidesAmirah Azman100% (4)
- D.A.V Senior Secondary School: Biology Investigatory ProjectDocument22 pagesD.A.V Senior Secondary School: Biology Investigatory ProjecthashimNo ratings yet
- Refractive DisorderDocument39 pagesRefractive Disorderalvi kamal fikriNo ratings yet
- Refractive Disorders Blok VisualDocument27 pagesRefractive Disorders Blok Visualmuhammad ajiNo ratings yet
- Physiology AccommodationDocument109 pagesPhysiology AccommodationAmmar bushraNo ratings yet
- FIXXXXXXDocument35 pagesFIXXXXXXRani Dwi HapsariNo ratings yet
- Decision MakingDocument8 pagesDecision MakingMuhammad LukmanNo ratings yet
- Cover Referat NeurologiDocument1 pageCover Referat NeurologiMuhammad LukmanNo ratings yet
- Baru Diedit DikitDocument20 pagesBaru Diedit DikitMuhammad LukmanNo ratings yet
- Antibiotic Misuse Among Children With Diarrhea in China - Dwi LestianaDocument2 pagesAntibiotic Misuse Among Children With Diarrhea in China - Dwi LestianaMuhammad LukmanNo ratings yet
- Genogram Pak TimbulDocument1 pageGenogram Pak TimbulMuhammad LukmanNo ratings yet
- Approach To DyspneaDocument9 pagesApproach To DyspneaMuhammad LukmanNo ratings yet
- Activity 5Document3 pagesActivity 5Muhammad LukmanNo ratings yet
- Sekretaris: No. Nama Barang Jumlah Harga Satuan Total HargaDocument4 pagesSekretaris: No. Nama Barang Jumlah Harga Satuan Total HargaMuhammad LukmanNo ratings yet
- Fiber Optic Communications Technology - D. K. Mynbaev and L. L. ScheinerDocument72 pagesFiber Optic Communications Technology - D. K. Mynbaev and L. L. Scheinerali raza100% (1)
- Mid Term-Ish Study GuideDocument3 pagesMid Term-Ish Study Guideapi-277921504No ratings yet
- Bell Ringer: Explain One of The Stations From Yesterday in DetailDocument77 pagesBell Ringer: Explain One of The Stations From Yesterday in DetailMark Jay BongolanNo ratings yet
- Designing Illumination OpticsDocument24 pagesDesigning Illumination OpticsGörkem VarolNo ratings yet
- DAC-004 Diode Line Camera Sensor Operating Manual: For Multi Edge Detection Using Virtual Scope Configuration SoftwareDocument33 pagesDAC-004 Diode Line Camera Sensor Operating Manual: For Multi Edge Detection Using Virtual Scope Configuration SoftwareEcaterina IrimiaNo ratings yet
- Dispersion Characteristics of Substrate IntegratedDocument3 pagesDispersion Characteristics of Substrate IntegratedUsman QureshiNo ratings yet
- Specification For SM Optical Fibre (G.657A) Low Bend: Aksh Optifibre LimitedDocument5 pagesSpecification For SM Optical Fibre (G.657A) Low Bend: Aksh Optifibre LimitedFfbFfbNo ratings yet
- Antenna FundamentalsDocument55 pagesAntenna FundamentalsMarco Aurelio PereiraNo ratings yet
- CLE LEA ReviewerDocument1,228 pagesCLE LEA ReviewerJan Edward CadizNo ratings yet
- Turbidez 1Document4 pagesTurbidez 1Mariana Karina Velasco AmadorNo ratings yet
- T4S4-90A-R2 Product SpecificationsDocument6 pagesT4S4-90A-R2 Product Specifications'Theodora GeorgianaNo ratings yet
- Chap.1. Brief HX & X-Ray ProductionDocument42 pagesChap.1. Brief HX & X-Ray ProductiongetemeselewNo ratings yet
- DWDMDocument33 pagesDWDMMahesh Kamath NNo ratings yet
- Ecss e ST 20 06C PDFDocument120 pagesEcss e ST 20 06C PDFBetsabé MNo ratings yet
- Physics Waves WorksheetDocument3 pagesPhysics Waves WorksheetRizky HermawanNo ratings yet
- Assessing The Reproducibility of Particle Size Measurements With MS3000Document5 pagesAssessing The Reproducibility of Particle Size Measurements With MS3000Victor FernandezNo ratings yet
- Science 7 - Summative TestDocument7 pagesScience 7 - Summative TestAbegail Panang100% (2)
- Aperture Antennas and LPDA1Document41 pagesAperture Antennas and LPDA1Innovative Smart learningNo ratings yet
- Michelson InterferometerDocument9 pagesMichelson InterferometerRico MahreziNo ratings yet
- 0625 TQ P3 Waves v2Document6 pages0625 TQ P3 Waves v2ammara shafiqueNo ratings yet
- Narrow-Band Filter For Satellite Communication SystemsDocument6 pagesNarrow-Band Filter For Satellite Communication SystemsIJICT JournalNo ratings yet
- Amity International School Noida CLASS X (2021-22) Ch. Light-Reflection & Refraction MLP Worksheet-2Document2 pagesAmity International School Noida CLASS X (2021-22) Ch. Light-Reflection & Refraction MLP Worksheet-2Anushka TripathiNo ratings yet
- AMO Sheet7Document3 pagesAMO Sheet7Ismael CastilloNo ratings yet
- Chirped PulseDocument2 pagesChirped PulseKapila WijayaratneNo ratings yet
- The Use of Remote Sensing To Locate Heavy Metal As Source of PollutionDocument18 pagesThe Use of Remote Sensing To Locate Heavy Metal As Source of PollutionМеруерт УлыкпановаNo ratings yet
- TutorialDocument104 pagesTutorialDaksh JainNo ratings yet
- Advent 1.2m SNG AntennaDocument2 pagesAdvent 1.2m SNG Antennaflorinf_uNo ratings yet
- ECE123Document7 pagesECE123Migz BorlonganNo ratings yet
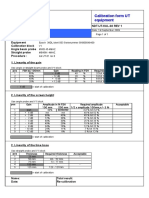
- Calibration Sheet Ultrasonic Test EquipmentDocument1 pageCalibration Sheet Ultrasonic Test EquipmentjohnNo ratings yet
- Brain HistoryDocument67 pagesBrain HistorySURAJIT DUTTANo ratings yet