You might also like
- Checklist: Mobile Crane SafetyDocument2 pagesChecklist: Mobile Crane SafetyJohn Kurong100% (5)
- SBI - Certificate To Be Submitted by Pensioner - ChandigarhDocument1 pageSBI - Certificate To Be Submitted by Pensioner - ChandigarhMsinghNo ratings yet
- Medical PhysicsDocument81 pagesMedical Physicsroni roniNo ratings yet
- S6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Document26 pagesS6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Rona Dindang100% (1)
- Physical Therapy Reduces Low Back PainDocument6 pagesPhysical Therapy Reduces Low Back PainAramanda DianNo ratings yet
- Piaggio MP3 300 Ibrido LT MY 2010 (En)Document412 pagesPiaggio MP3 300 Ibrido LT MY 2010 (En)Manualles100% (3)
- Understanding Musculoskeletal TumoursDocument106 pagesUnderstanding Musculoskeletal TumoursBharath NarasimhaNo ratings yet
- Chronic OsteomyelitisDocument29 pagesChronic OsteomyelitisAbdul BasitNo ratings yet
- Bone Tumor: Daniel A. (Orthopedic Surgeon)Document225 pagesBone Tumor: Daniel A. (Orthopedic Surgeon)mebrieNo ratings yet
- Temporo Mandibular Joint Disorder Oral SurgeryDocument59 pagesTemporo Mandibular Joint Disorder Oral SurgeryFourthMolar.comNo ratings yet
- 6.musculoskeletal TumorsDocument110 pages6.musculoskeletal Tumorslina jamalNo ratings yet
- Bone and Joint TumoursDocument49 pagesBone and Joint TumoursMahmoud Abu Al Amrain100% (1)
- Jurnal SinusitisDocument49 pagesJurnal SinusitisAramanda Dian100% (1)
- Consider Recycled Water PDFDocument0 pagesConsider Recycled Water PDFAnonymous 1XHScfCINo ratings yet
- Handbook For Magnaflux L10 CoilDocument4 pagesHandbook For Magnaflux L10 CoilmgmqroNo ratings yet
- Temporomandibular Joint DiseaseDocument84 pagesTemporomandibular Joint Diseaseapi-19916399No ratings yet
- 01 Slug CatchersDocument23 pages01 Slug CatchersMohamed Sahnoun100% (2)
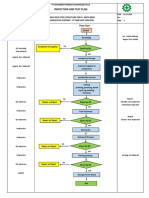
- Inspection and Test Plan: Flow Chart Start IncomingDocument1 pageInspection and Test Plan: Flow Chart Start IncomingSinden AyuNo ratings yet
- Management of Temporomandibular Joint AnkylosisDocument40 pagesManagement of Temporomandibular Joint AnkylosisluthfiazharisaniNo ratings yet
- 06wk48 - CSSR Improvement Fach Power Trial Phase II - VDF UKDocument19 pages06wk48 - CSSR Improvement Fach Power Trial Phase II - VDF UKsyedNo ratings yet
- NEOPLASMA of MUSCULOSKELETAL TISSUES (boneDocument19 pagesNEOPLASMA of MUSCULOSKELETAL TISSUES (boneRizqon Yassir KuswondoNo ratings yet
- Musculoskeletal Tumor Management Clinical Staging and Treatment PlanningDocument16 pagesMusculoskeletal Tumor Management Clinical Staging and Treatment PlanningRonald TejoprayitnoNo ratings yet
- The Most Common Primary Malignant Tumor of The BoneDocument28 pagesThe Most Common Primary Malignant Tumor of The BoneandhitaNo ratings yet
- Musculoskeletal tumor classification and treatmentDocument89 pagesMusculoskeletal tumor classification and treatmentHayaNo ratings yet
- Anatomy of The Upper and Lower Extremities Neoplasms of MusculosDocument93 pagesAnatomy of The Upper and Lower Extremities Neoplasms of MusculosraihanekapNo ratings yet
- Orthopedics 5 Year SolveDocument5 pagesOrthopedics 5 Year SolveChowdhury Mohammed Tawhid TasneefNo ratings yet
- Bone and Joint Neoplasm or TumorDocument49 pagesBone and Joint Neoplasm or Tumorendah rahmadaniNo ratings yet
- Musculoskeletal Neoplasms GuideDocument21 pagesMusculoskeletal Neoplasms Guidei dewa wisnu putraNo ratings yet
- Bone TumorsDocument6 pagesBone Tumorsa179360No ratings yet
- Spinal Tumor StrongDocument45 pagesSpinal Tumor StrongbettyNo ratings yet
- Cranium 3Document26 pagesCranium 3giant nitaNo ratings yet
- Primary Spinal Tumour Classification and Surgical ConsiderationsDocument5 pagesPrimary Spinal Tumour Classification and Surgical ConsiderationsLyneth LacourtNo ratings yet
- PATH - Bony Tumours (6p)Document6 pagesPATH - Bony Tumours (6p)andreeaNo ratings yet
- Bone Tumors: - Most Common:: 5-Minute Orthopaedic Consult, 2nd EditionDocument20 pagesBone Tumors: - Most Common:: 5-Minute Orthopaedic Consult, 2nd EditionNiqavie IndonesiaNo ratings yet
- Bone Scintigraphy in Primary Malignant Bone Tumor: CreutzigDocument2 pagesBone Scintigraphy in Primary Malignant Bone Tumor: Creutziglina huraibyNo ratings yet
- Principle of Bone Tumor DiagnosisDocument11 pagesPrinciple of Bone Tumor Diagnosisalimran MahmudNo ratings yet
- Classification and Treatment of Bone TumorsDocument6 pagesClassification and Treatment of Bone TumorsRonald TejoprayitnoNo ratings yet
- Chronic Osteomyelitis: Dr. F. Abdul Khader Professor & HOD Department of Orthopaedics SSSMC & RiDocument31 pagesChronic Osteomyelitis: Dr. F. Abdul Khader Professor & HOD Department of Orthopaedics SSSMC & RiDr. F. Abdul KhaderNo ratings yet
- Low-Grade Osteosarcoma of The MandibleDocument5 pagesLow-Grade Osteosarcoma of The MandibleGalih AryyagunawanNo ratings yet
- Bone Tumor Seminar: Types & ManagementDocument80 pagesBone Tumor Seminar: Types & ManagementPATHMAPRIYA GANESANNo ratings yet
- UU 5 1997psikotropikaDocument85 pagesUU 5 1997psikotropikaMeilina PutriNo ratings yet
- حل اسئلة العملي-1Document91 pagesحل اسئلة العملي-1حسام الوجيهNo ratings yet
- Lupus Case Study Part 3Document20 pagesLupus Case Study Part 3Mykee SuizoNo ratings yet
- Osteosarcoma & Ewin's SarcomaDocument34 pagesOsteosarcoma & Ewin's SarcomaAbdulMushibNo ratings yet
- Update A1 OsceDocument120 pagesUpdate A1 OsceIndra SetyaNo ratings yet
- Tumor MusculoskeletalDocument41 pagesTumor Musculoskeletalrisky setyanNo ratings yet
- 1 s2.0 S2049080122008718 MainDocument4 pages1 s2.0 S2049080122008718 MainFarizka Dwinda HidayatNo ratings yet
- Radio Logical Assessment of OA FinalDocument60 pagesRadio Logical Assessment of OA FinaltarikeopsNo ratings yet
- Clinical Data: Numerous Nevoid Pigmented Papules On Sun-Exposed and Sun-Protected Skin, Starting in Adolescence Case 1Document17 pagesClinical Data: Numerous Nevoid Pigmented Papules On Sun-Exposed and Sun-Protected Skin, Starting in Adolescence Case 1dr_RMNo ratings yet
- Osteochondroma of The Coronoid Process of The MandibleDocument4 pagesOsteochondroma of The Coronoid Process of The MandiblegtawidhiNo ratings yet
- Jaw Tumors: DR - Sudipta Bera PDT 1 Year Plastic and Reconstructive Surgery SSKM & IpgmerDocument28 pagesJaw Tumors: DR - Sudipta Bera PDT 1 Year Plastic and Reconstructive Surgery SSKM & Ipgmerdevinchi09No ratings yet
- Neoplasm On Bone and Soft Tissue MikoDocument151 pagesNeoplasm On Bone and Soft Tissue Mikoindra muhammadNo ratings yet
- MBD Referat: Metastatic Bone Disease Pathogenesis, Diagnosis, and TreatmentDocument25 pagesMBD Referat: Metastatic Bone Disease Pathogenesis, Diagnosis, and Treatmentanggita tri yurisworoNo ratings yet
- Dr. Ronald V. Munthe Spot SMF Bedah Rs UkiDocument50 pagesDr. Ronald V. Munthe Spot SMF Bedah Rs UkiOdilia Maria RahalusNo ratings yet
- Pathology of Musculoskeletal System: Bone Tumors and DiseasesDocument68 pagesPathology of Musculoskeletal System: Bone Tumors and DiseaseswilliamNo ratings yet
- GCG Palate PDC 15 - 4 - 135Document5 pagesGCG Palate PDC 15 - 4 - 135Yiu Kai WongNo ratings yet
- JCM 11 00166 With CoverDocument29 pagesJCM 11 00166 With CoverBruno MañonNo ratings yet
- JointsDocument68 pagesJointsLaine ZeeNo ratings yet
- Maloney 2021Document25 pagesMaloney 2021ShathaNo ratings yet
- Infected Non Union1Document41 pagesInfected Non Union1SyarifNo ratings yet
- Transverse Myelitis AtfDocument3 pagesTransverse Myelitis AtfRishi VermaNo ratings yet
- Open and Closed Fractures - 2018 EnglishDocument49 pagesOpen and Closed Fractures - 2018 EnglishЕлена КовбасаNo ratings yet
- Dolwick2012 PDFDocument10 pagesDolwick2012 PDFpaolaNo ratings yet
- Non-Neoplastic Bone Disease GuideDocument45 pagesNon-Neoplastic Bone Disease GuideKNo ratings yet
- Epithelioid Sarcoma of The Big Toe: A Case ReportDocument4 pagesEpithelioid Sarcoma of The Big Toe: A Case ReportIlincaNo ratings yet
- Myositis Ossificans in The Infraspinatus Muscle: The Key To DiagnosisDocument3 pagesMyositis Ossificans in The Infraspinatus Muscle: The Key To DiagnosisNabil Sangga BuanaNo ratings yet
- Malignant Bone TumoursDocument38 pagesMalignant Bone Tumoursgdudex118811No ratings yet
- (MED) F.22 Polymyositis, Dermatomyositis (Reading Assignment)Document6 pages(MED) F.22 Polymyositis, Dermatomyositis (Reading Assignment)Yves RamosNo ratings yet
- 3 Essay OrthoDocument11 pages3 Essay Orthogamal attamNo ratings yet
- Fulltext - Smjo v3 1059Document3 pagesFulltext - Smjo v3 1059Rachell AchellNo ratings yet
- Surgery of the Cranio-Vertebral JunctionFrom EverandSurgery of the Cranio-Vertebral JunctionEnrico TessitoreNo ratings yet
- CBD Case DiscussionDocument35 pagesCBD Case DiscussionAramanda DianNo ratings yet
- AlbertusDocument15 pagesAlbertusAramanda DianNo ratings yet
- Bone Tumor - Dr. Andri R. Winoto, SpOT (K)Document19 pagesBone Tumor - Dr. Andri R. Winoto, SpOT (K)Aramanda DianNo ratings yet
- 10 1093@jac@dky006Document5 pages10 1093@jac@dky006Aramanda DianNo ratings yet
- 10 1093@jac@dky006Document5 pages10 1093@jac@dky006Aramanda DianNo ratings yet
- ReferenceDocument3 pagesReferenceAramanda DianNo ratings yet
- Product GuideDocument13 pagesProduct Guidekhalid mostafaNo ratings yet
- Eu Donor Atlas PDFDocument2 pagesEu Donor Atlas PDFBrentNo ratings yet
- RESEARCH PROPOSAL-Final AfraaaazzzzzzzzzDocument13 pagesRESEARCH PROPOSAL-Final AfraaaazzzzzzzzzRizwan Abdul Maalik50% (2)
- Pakistan List of Approved Panel PhysicianssDocument5 pagesPakistan List of Approved Panel PhysicianssGulzar Ahmad RawnNo ratings yet
- PR Cuisine vs US CuisineDocument2 pagesPR Cuisine vs US CuisineJannette HernandezNo ratings yet
- DOC023.97.80076 - 3ed Sensores ORPDocument148 pagesDOC023.97.80076 - 3ed Sensores ORPAlejandroNo ratings yet
- Jamec Air FittingsDocument18 pagesJamec Air Fittingsgoeez1No ratings yet
- Practical Research 1 Quarter 1 - Module 10: Through The SlateDocument10 pagesPractical Research 1 Quarter 1 - Module 10: Through The SlateMark Allen Labasan100% (1)
- Concept PaperDocument6 pagesConcept Paperapple amanteNo ratings yet
- Olpers MilkDocument4 pagesOlpers MilkARAAJ YOUSUFNo ratings yet
- 9 Oet Reading Summary 2.0-195-213Document19 pages9 Oet Reading Summary 2.0-195-213Vijayalakshmi Narayanaswami0% (1)
- INFORSHT Produktkatalog en Web 03.22Document13 pagesINFORSHT Produktkatalog en Web 03.22lolNo ratings yet
- Batson Et All - 2007 - Anger and Unfairness - Is It Moral Outrage?Document15 pagesBatson Et All - 2007 - Anger and Unfairness - Is It Moral Outrage?Julia GonzalezNo ratings yet
- Causes of DyspneaDocument9 pagesCauses of DyspneaHanis Afiqah Violet MeowNo ratings yet
- Acute Coronary Syndrome Guidelines 2020Document79 pagesAcute Coronary Syndrome Guidelines 2020Γιώργος ΕλευθεριάδηςNo ratings yet
- Human Diseases A Systemic Approach 8th Edition-Páginas-15-26Document12 pagesHuman Diseases A Systemic Approach 8th Edition-Páginas-15-26Karime LopezNo ratings yet
- Limetas Maximos ResidualesDocument27 pagesLimetas Maximos ResidualesXjoelx Olaya GonzalesNo ratings yet
- Undas Deployment PadsDocument15 pagesUndas Deployment PadsVic NairaNo ratings yet
- Environmental Science OEdDocument9 pagesEnvironmental Science OEdGenevieve AlcantaraNo ratings yet
- 1324 1624 1824 Owners Manual 6 4 08Document64 pages1324 1624 1824 Owners Manual 6 4 08Miguel LopNo ratings yet