You might also like
- When The Air Hits Your BrainDocument197 pagesWhen The Air Hits Your BrainTest100% (2)
- Ostpartum Hemorrhage: Dr. Patiyus Agustiansyah, Spog (K)Document70 pagesOstpartum Hemorrhage: Dr. Patiyus Agustiansyah, Spog (K)JoNo ratings yet
- Gallstones in Pregnancy - UpToDateDocument51 pagesGallstones in Pregnancy - UpToDateLeira BarbosaNo ratings yet
- Queenan's Management of High-Risk Pregnancy: An Evidence-Based ApproachFrom EverandQueenan's Management of High-Risk Pregnancy: An Evidence-Based ApproachNo ratings yet
- MSI Guidelines For Obstetric Care v2.0Document295 pagesMSI Guidelines For Obstetric Care v2.0Daniel AbomaNo ratings yet
- Disseminated Intravascular Coagulation: Keith Lewis, MDDocument37 pagesDisseminated Intravascular Coagulation: Keith Lewis, MDRitamaria100% (1)
- Myoma UteriDocument8 pagesMyoma UteriFaraida Arvilla100% (1)
- Gestational Trophoblastic DiseaseDocument58 pagesGestational Trophoblastic DiseaseJalajarani SelvaNo ratings yet
- Antiphospholipid Syndrome in PregnancyDocument7 pagesAntiphospholipid Syndrome in PregnancyDara Dasawulansari SyamsuriNo ratings yet
- Gynecological History Taking and ExaminationDocument17 pagesGynecological History Taking and Examinationnmsiswaridewi100% (1)
- PPH 2024Document25 pagesPPH 2024Anthony Mwangi100% (1)
- Abnormal OBDocument34 pagesAbnormal OBLawrence NemirNo ratings yet
- Ovarian Cysts and Cancer in PregnancyDocument15 pagesOvarian Cysts and Cancer in Pregnancykarina100% (1)
- Abnormal Uterine BleedingDocument12 pagesAbnormal Uterine BleedingGilang DermawanNo ratings yet
- OB Lec ArellanoDocument834 pagesOB Lec Arellanoervin_agena394No ratings yet
- Hydatidiform MoleDocument10 pagesHydatidiform MoleLisa TurnerNo ratings yet
- Idiophatic Thrombocytopenic Purpura (ITP) in PregnancyDocument27 pagesIdiophatic Thrombocytopenic Purpura (ITP) in PregnancyAdietya Bima PrakasaNo ratings yet
- Hypertension in PregnancyDocument34 pagesHypertension in PregnancyMusekhirNo ratings yet
- Uterus NeoDocument11 pagesUterus NeoHester Marie SimpiaNo ratings yet
- Postpartum HemorrhageDocument20 pagesPostpartum Hemorrhagem_amroellahNo ratings yet
- Ectopic PregnancyDocument5 pagesEctopic PregnancyFaith FuentevillaNo ratings yet
- A Nursing Case Study On EctopicPregnancy PDFDocument60 pagesA Nursing Case Study On EctopicPregnancy PDFSteffiNo ratings yet
- Multiple Pregnancy: Dr. A. Farid Abdullah, SP - OG, M.KesDocument33 pagesMultiple Pregnancy: Dr. A. Farid Abdullah, SP - OG, M.KesAndi Farid ANo ratings yet
- Acute GlomerulonephritisDocument28 pagesAcute GlomerulonephritisPaul SinsNo ratings yet
- Hypertensive Disorders in Pregnancy: Maisuri T. ChalidDocument44 pagesHypertensive Disorders in Pregnancy: Maisuri T. ChalidinhaNo ratings yet
- Endometrial Hyperplasia: by Dr. Mervat AliDocument48 pagesEndometrial Hyperplasia: by Dr. Mervat AliAsh AmeNo ratings yet
- Hepatitis B in PregnancyDocument17 pagesHepatitis B in PregnancysnazzyNo ratings yet
- Abruptio Placentae: Insert or Drag & Drop Your PhotoDocument42 pagesAbruptio Placentae: Insert or Drag & Drop Your PhotoClareen JuanicoNo ratings yet
- Φ PathophysiologyDocument4 pagesΦ PathophysiologyMariah AshooriyanNo ratings yet
- Impey Obs and Gynae Revision Notes PDFDocument9 pagesImpey Obs and Gynae Revision Notes PDFRoiseNo ratings yet
- Assisted Reproductive TechniquesDocument146 pagesAssisted Reproductive TechniquesGouravNo ratings yet
- Abruptio PlacentaDocument4 pagesAbruptio PlacentaChelzie LasernaNo ratings yet
- Abruptio Placenta B-1Document29 pagesAbruptio Placenta B-1drsachinhNo ratings yet
- Antenatal Obstetric ComplicationsDocument40 pagesAntenatal Obstetric ComplicationsArhum SiddiqiNo ratings yet
- Gestational Hypertension-MeDocument32 pagesGestational Hypertension-Mekurt94764No ratings yet
- Pelvic Inflammatory DiseaseDocument26 pagesPelvic Inflammatory DiseaseMelati Setia Ningsih100% (1)
- Amniotic Fluid Embolism (AFE)Document26 pagesAmniotic Fluid Embolism (AFE)sanjivdas100% (1)
- Revision Long Case Obs GynaeDocument10 pagesRevision Long Case Obs GynaeHo Yong WaiNo ratings yet
- Dr. Sharda Jain: Director: Secretary GeneralDocument91 pagesDr. Sharda Jain: Director: Secretary GeneraljijaniNo ratings yet
- BENIGN OVARIAN DISEASES - Updated January 2018Document31 pagesBENIGN OVARIAN DISEASES - Updated January 2018daniel100% (1)
- PBL Report 3 FixDocument24 pagesPBL Report 3 FixtiwiNo ratings yet
- Gestational Trophoblastic Disease: (Hydatidiform Mole)Document12 pagesGestational Trophoblastic Disease: (Hydatidiform Mole)Gylle Marie PlazaNo ratings yet
- Perio - Biofilm and Periodontal Microbiology (Without Tables) - MergedDocument11 pagesPerio - Biofilm and Periodontal Microbiology (Without Tables) - MergedGlyndale CatalunaNo ratings yet
- AMTSL BrieferDocument2 pagesAMTSL BrieferNewborn2013No ratings yet
- 1 - Presentation - Management of Preclamplsia, Mild and ModerateDocument22 pages1 - Presentation - Management of Preclamplsia, Mild and ModeratesharonNo ratings yet
- Postpartum CollapseDocument54 pagesPostpartum Collapsemedical chroniclesNo ratings yet
- Abnormalities of The Passage-WilliamsDocument66 pagesAbnormalities of The Passage-Williamsapi-19641337100% (1)
- Ectopic Pregnancy1Document34 pagesEctopic Pregnancy1Kreshimaricon FurigayNo ratings yet
- Poly and OligohydramniosDocument39 pagesPoly and OligohydramniosMohamed Atef MohamedNo ratings yet
- Complications During Pregnancy - Chapt 5Document93 pagesComplications During Pregnancy - Chapt 5klyde_evangelistaNo ratings yet
- OSCE Revision OBG DocumentDocument60 pagesOSCE Revision OBG DocumentshreyaNo ratings yet
- Endometrial HyperplasiaDocument12 pagesEndometrial HyperplasiaHenri KnafoNo ratings yet
- Sakila MurmuDocument47 pagesSakila MurmuSakila murmuNo ratings yet
- Hypertension in Pregnancy-LatestDocument32 pagesHypertension in Pregnancy-LatestshahiraazNo ratings yet
- Gestational Trophoblastic Disease Pt2Document75 pagesGestational Trophoblastic Disease Pt2yurie_ameliaNo ratings yet
- Hypertension Lecture For Cci 2013Document74 pagesHypertension Lecture For Cci 2013Hannie CruelNo ratings yet
- Preterm Prelabour Rupture of MembranesDocument12 pagesPreterm Prelabour Rupture of MembranesSeptiany Indahsari DjanNo ratings yet
- O and G Notes Notebank NumberedDocument173 pagesO and G Notes Notebank NumberedPerscitus Ali القحطانيNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- ACGGuideline Liver Disease and Pregnancy 2016 PDFDocument19 pagesACGGuideline Liver Disease and Pregnancy 2016 PDFArnella HutagalungNo ratings yet
- ACGGuideline Liver Disease and Pregnancy 2016 PDFDocument19 pagesACGGuideline Liver Disease and Pregnancy 2016 PDFArnella HutagalungNo ratings yet
- 4 EngDocument209 pages4 Engbjfiero100% (1)
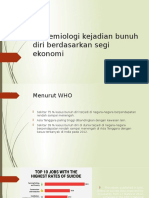
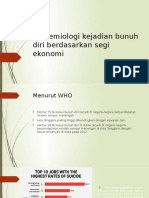
- Epidemiologi Kejadian Bunuh Diri Berdasarkan Segi EkonomiDocument3 pagesEpidemiologi Kejadian Bunuh Diri Berdasarkan Segi EkonomiGabbyNo ratings yet
- Epidemiologi Kejadian Bunuh Diri Berdasarkan Segi EkonomiDocument3 pagesEpidemiologi Kejadian Bunuh Diri Berdasarkan Segi EkonomiGabbyNo ratings yet
- Mother Earth BackDocument1 pageMother Earth BackGabbyNo ratings yet
- Issue 3 Dennis Slater Dear Directors LetterDocument1 pageIssue 3 Dennis Slater Dear Directors Letterapi-400507461No ratings yet
- Urological History & ExaminationDocument44 pagesUrological History & ExaminationswlocoNo ratings yet
- Acute Appendicitis Made EasyDocument8 pagesAcute Appendicitis Made EasyTakpire DrMadhukarNo ratings yet
- BPH and Prostate Cancer 11Document225 pagesBPH and Prostate Cancer 11Blessy MadhuriNo ratings yet
- Operational Guidelines For Establishing Sentinel Stillbirth Surveillance SystemDocument40 pagesOperational Guidelines For Establishing Sentinel Stillbirth Surveillance Systemraval anil.uNo ratings yet
- Prostate Cancer AwarenessDocument10 pagesProstate Cancer AwarenessarthurmathieuNo ratings yet
- ICOEDocument2 pagesICOEmeutia wardhanie ganieNo ratings yet
- MAMC B.sc. Nursing ProspectusDocument24 pagesMAMC B.sc. Nursing ProspectusMota Chashma100% (2)
- Case Report: Viona I11109064Document41 pagesCase Report: Viona I11109064DiskaAstariniNo ratings yet
- Jaundice in PregnancyDocument32 pagesJaundice in PregnancyManoj Sankaranarayana100% (2)
- Ophthalmic Surgeon in HKDocument4 pagesOphthalmic Surgeon in HKJOHAYNIENo ratings yet
- Obstetric Abdominal Examination OSCE GuideDocument16 pagesObstetric Abdominal Examination OSCE GuideMuhammad Aamir IqbalNo ratings yet
- Evaluation of The Hip: History, Physical Examination, and ImagingDocument11 pagesEvaluation of The Hip: History, Physical Examination, and ImagingmilelytaNo ratings yet
- Caso 1 Six SigmaDocument9 pagesCaso 1 Six SigmaNayibe Tatiana Sanchez AlvarezNo ratings yet
- Respectful Maternity CareDocument33 pagesRespectful Maternity CareJenelle Melinda TullochNo ratings yet
- Minor Discomfort and Complication Puerperium Topic FINALDocument14 pagesMinor Discomfort and Complication Puerperium Topic FINALsuman guptaNo ratings yet
- Materi Sampai Uts FinalDocument35 pagesMateri Sampai Uts FinalNur HidayantiNo ratings yet
- (2017) Bladder BrachyDocument7 pages(2017) Bladder BrachyStirNo ratings yet
- HEALTH REAC 4 Physicians by CategoriesDocument43 pagesHEALTH REAC 4 Physicians by CategoriesMahmoudNo ratings yet
- Insights Into Veterinary Endocrinology - Diagnostic Approach To PU - PD - Urine Specific GravityDocument4 pagesInsights Into Veterinary Endocrinology - Diagnostic Approach To PU - PD - Urine Specific GravityHusnat hussainNo ratings yet
- Mayo Paediatricians Manual 4th EdDocument153 pagesMayo Paediatricians Manual 4th EdFalah NadeemNo ratings yet
- Statement of Purpose (Clinical Dermatology-MSc) Cardiff UniversityDocument3 pagesStatement of Purpose (Clinical Dermatology-MSc) Cardiff UniversitySheikh Shafiq Siam100% (1)
- EsoDocument2 pagesEsoChristopherFernandoSapíenDelgadoNo ratings yet
- Nursing Medical AbbreviationDocument7 pagesNursing Medical AbbreviationJoan Claire R. YbanezNo ratings yet
- Anaesthesia: Update inDocument7 pagesAnaesthesia: Update inhabtishNo ratings yet
- Philiphs HD7 Brochure - UltrasoundDocument6 pagesPhiliphs HD7 Brochure - UltrasoundIvan CvasniucNo ratings yet
- Articaine in Oral SurgeryDocument19 pagesArticaine in Oral SurgeryAimeeNo ratings yet
- 2004, Vol.31, Issues 1, Ultrasound in ObstetricsDocument213 pages2004, Vol.31, Issues 1, Ultrasound in ObstetricsFebrinata MahadikaNo ratings yet
- Challenges in Fertility Regulation - Multiple Choice Questions Only For Vol. 28, No. 6 - Obgyn KeyDocument1 pageChallenges in Fertility Regulation - Multiple Choice Questions Only For Vol. 28, No. 6 - Obgyn Keyabdelrazag T GhadbanNo ratings yet