You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Lampiran SMA Papua BaratDocument21 pagesLampiran SMA Papua Baratputri auliyahNo ratings yet
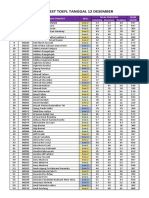
- Hasil Test TOEFL 12 DesemberDocument12 pagesHasil Test TOEFL 12 Desemberputri auliyahNo ratings yet
- Dxy Manejo Histiocitosis DR Gomez RezaDocument10 pagesDxy Manejo Histiocitosis DR Gomez Rezaputri auliyahNo ratings yet
- Prevensi Allergy Blok 20 Maret 2013 PDFDocument27 pagesPrevensi Allergy Blok 20 Maret 2013 PDFputri auliyahNo ratings yet
- Jurnal 1Document6 pagesJurnal 1putri auliyahNo ratings yet
- Jurnal 3Document9 pagesJurnal 3putri auliyahNo ratings yet
- Diagnosis and Mangement of Skin Allergy DiseasesDocument14 pagesDiagnosis and Mangement of Skin Allergy Diseasesputri auliyahNo ratings yet
- Neuro4Nurses Acustic NeuromaDocument2 pagesNeuro4Nurses Acustic Neuromaputri auliyahNo ratings yet
- Diagnosis & Management of Anaphylactic Shock NewDocument6 pagesDiagnosis & Management of Anaphylactic Shock Newputri auliyahNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pyoderma GangrenosumDocument35 pagesPyoderma GangrenosumkylieverNo ratings yet
- The Emerging Field of Human Social GenomicsDocument18 pagesThe Emerging Field of Human Social GenomicsEdilson RodriguesNo ratings yet
- Ubogu - Inflammatory NeuropathiesDocument24 pagesUbogu - Inflammatory NeuropathiesMarcelo BedoyaNo ratings yet
- COVID - 19 and Cancer: Priyanka Joshi Chhandasri TarangDocument7 pagesCOVID - 19 and Cancer: Priyanka Joshi Chhandasri TarangLisa MishraNo ratings yet
- Yogic Cure For ArthritiesDocument59 pagesYogic Cure For Arthritiesstar893190No ratings yet
- Curcumin c3 Complex PDFDocument7 pagesCurcumin c3 Complex PDFGopalaKrishnan Sivaraman0% (1)
- Dry Eyes Drug TreatmentDocument3 pagesDry Eyes Drug Treatmentlu100% (1)
- Pulp CappingDocument59 pagesPulp Cappingதிருவேங்கடம் கோபாலன்No ratings yet
- Part I June 2013: 1. 1-The Physiological Dead SpaceDocument20 pagesPart I June 2013: 1. 1-The Physiological Dead SpaceHazim Rhman AliNo ratings yet
- Leukogram Patterns - EClinpathDocument6 pagesLeukogram Patterns - EClinpathCarlos YongNo ratings yet
- Ch2 InflamDocument49 pagesCh2 InflamleartaNo ratings yet
- Inflammation & Repair PDFDocument33 pagesInflammation & Repair PDFsri astuti100% (1)
- Isicem 2021Document90 pagesIsicem 2021labbeneNo ratings yet
- Nursing Care of Clients With Immunologic Disorders: Immune SystemDocument7 pagesNursing Care of Clients With Immunologic Disorders: Immune SystemIrish Eunice FelixNo ratings yet
- Morpho - Pathology Final Summary: Chapter 1: Cellular Reactions To AggressionDocument21 pagesMorpho - Pathology Final Summary: Chapter 1: Cellular Reactions To Aggressiondjxela89No ratings yet
- Repair and Regeneration of Oral Tissues - Ten Cate Chapter 15Document3 pagesRepair and Regeneration of Oral Tissues - Ten Cate Chapter 15Chris Tay100% (2)
- Endometriosis PathophysiologyDocument4 pagesEndometriosis PathophysiologyGeLa GutierrezNo ratings yet
- Jaco Malan Drops CardsDocument10 pagesJaco Malan Drops Cardsjojo 9000No ratings yet
- Immunopathogenesis of Pelvic en Dome Trios Is - Role of Hepatocyte Growth Factor, Macrophages and Ovarian SteroidsDocument23 pagesImmunopathogenesis of Pelvic en Dome Trios Is - Role of Hepatocyte Growth Factor, Macrophages and Ovarian SteroidsJessi WinklerNo ratings yet
- Host and Environmental Factors Influencing Individual Human Cytokine Responses PDFDocument37 pagesHost and Environmental Factors Influencing Individual Human Cytokine Responses PDFLluis GomezNo ratings yet
- Nonmalignant WBC DisordersDocument7 pagesNonmalignant WBC DisordersHarvey Mher Rarang100% (3)
- Oral Versus Topical NSAIDs in Rheumatic DiseasesDocument21 pagesOral Versus Topical NSAIDs in Rheumatic DiseasesAnonymous so6ZnlKywNo ratings yet
- NCM 112 TH (12F)Document24 pagesNCM 112 TH (12F)Justine April YbanezNo ratings yet
- Neutrophils-Lymphocytes Ratio (NLR) and Platelet-Lymphocytes Ratio (PLR) As Predictors of NSTEMI EventDocument9 pagesNeutrophils-Lymphocytes Ratio (NLR) and Platelet-Lymphocytes Ratio (PLR) As Predictors of NSTEMI EventYohanes FirmansyahNo ratings yet
- Resistencia A La Insulina - 14-1149239Document24 pagesResistencia A La Insulina - 14-1149239Marcelo TrNo ratings yet
- Nampath MonositDocument8 pagesNampath MonositEllya Latifah IlyasNo ratings yet
- Pulpal IrritantsDocument10 pagesPulpal IrritantsDiverse AnunturiNo ratings yet
- 10 Essentials To Improving EyesightDocument9 pages10 Essentials To Improving Eyesightdrakpo100% (1)
- 1 s2.0 S0753332217349909 MainDocument11 pages1 s2.0 S0753332217349909 MainBadiu ElenaNo ratings yet
- Adalimumab PIDocument31 pagesAdalimumab PIWei Sheng ChongNo ratings yet