You might also like
- Book Eczema PsoriazisDocument457 pagesBook Eczema Psoriazisdaniel bNo ratings yet
- Neurology, Neurosurgery MCQ PointsDocument32 pagesNeurology, Neurosurgery MCQ PointsBruno86% (7)
- DR AKASH Thesis PDFDocument97 pagesDR AKASH Thesis PDFAkash SinghalNo ratings yet
- Family Case Study For HydrocephalusDocument9 pagesFamily Case Study For HydrocephalusjaegergranNo ratings yet
- NEET PG 2013 Rank List of Eligible CandidatesDocument256 pagesNEET PG 2013 Rank List of Eligible CandidatesBruno75% (8)
- Chapter 7 Africa South of The SaharaDocument40 pagesChapter 7 Africa South of The Saharafuck ypouNo ratings yet
- Nursing Diagnosis For AsthmaDocument6 pagesNursing Diagnosis For AsthmaTINAIDA33% (3)
- GAD Database DCFDocument26 pagesGAD Database DCFBaby Jane Dedase100% (1)
- Accessibility and Quality of Health Care ServicesDocument69 pagesAccessibility and Quality of Health Care Servicesyra capili100% (1)
- Prof DR Amit Gupta AITSC Trauma Registry & Trauma Quality Improvement in IndiaDocument77 pagesProf DR Amit Gupta AITSC Trauma Registry & Trauma Quality Improvement in IndiaBruno50% (2)
- Zbornik Limes Vol 2Document354 pagesZbornik Limes Vol 2Morrigan100% (1)
- Basics of DentistryDocument65 pagesBasics of DentistryHiba Shah100% (1)
- Diagnostics 12 01289Document15 pagesDiagnostics 12 01289Sushmica BaquiranNo ratings yet
- 1 s2.0 S1008127516302735 MainDocument6 pages1 s2.0 S1008127516302735 MainAyu AzrinaNo ratings yet
- Prof DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesDocument42 pagesProf DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesBrunoNo ratings yet
- Functional Outcome of Trochanteric Fixation Nail Treatment in Elderly Patients With Intertrochanteric Femur FractureDocument8 pagesFunctional Outcome of Trochanteric Fixation Nail Treatment in Elderly Patients With Intertrochanteric Femur FractureIJAR JOURNALNo ratings yet
- Arthroplasty Today: Christopher F. Deans, MD, Leonard T. Buller, MD, Mary Ziemba-Davis, BA, R. Michael Meneghini, MDDocument6 pagesArthroplasty Today: Christopher F. Deans, MD, Leonard T. Buller, MD, Mary Ziemba-Davis, BA, R. Michael Meneghini, MDSanty OktavianiNo ratings yet
- A Prospective Descriptive Study of Trauma Registry in Netaji Subhash Chandra Bose Medical College, JabalpurDocument9 pagesA Prospective Descriptive Study of Trauma Registry in Netaji Subhash Chandra Bose Medical College, JabalpurIJAR JOURNALNo ratings yet
- Pico EbrDocument6 pagesPico Ebrapi-532699584No ratings yet
- Ess20 BPS Ssi Wuk FinalDocument18 pagesEss20 BPS Ssi Wuk FinaldynararakelNo ratings yet
- ORNDocument9 pagesORNsiddhi bhojakNo ratings yet
- Mehu 108 U3 T6 EpidmiologicalcharacteristicsDocument12 pagesMehu 108 U3 T6 EpidmiologicalcharacteristicsPedro PeredaNo ratings yet
- Nurul Khotifah (1811122) Judul SkripsiDocument32 pagesNurul Khotifah (1811122) Judul SkripsiNurul KhotifahNo ratings yet
- 2017 07 12 IV Catheter Securement Tech EB Best Pract N VideoDocument42 pages2017 07 12 IV Catheter Securement Tech EB Best Pract N VideoUbay GendulNo ratings yet
- 3 DBioprintingDocument10 pages3 DBioprintingDjordje DjordjevicNo ratings yet
- Australian - 2008 - Maxillofacial Trauma in Major Trauma PatientsDocument6 pagesAustralian - 2008 - Maxillofacial Trauma in Major Trauma Patientsووويويويةءتؤوبةين للاNo ratings yet
- Devendra 2020Document10 pagesDevendra 2020andiNo ratings yet
- uNA LESION POCO COMUN LESION CADENA DE MOTODocument7 pagesuNA LESION POCO COMUN LESION CADENA DE MOTOOscar Cayetano Herrera RodríguezNo ratings yet
- Journal of Orthopaedics: Anil K. Bhat, Siddarth Kamath KDocument7 pagesJournal of Orthopaedics: Anil K. Bhat, Siddarth Kamath KDita AldiniNo ratings yet
- 491-Article Text-2112-1-10-20210716Document6 pages491-Article Text-2112-1-10-20210716Dhimas Aji RadityaNo ratings yet
- Module 1 - Ardagh Et Al (2012)Document7 pagesModule 1 - Ardagh Et Al (2012)endroNo ratings yet
- Sciadv Ade7007Document11 pagesSciadv Ade7007Poramate PITAK-ARNNOPNo ratings yet
- Helix Alliance - Resume (Dr. Appukutty Manickam (Kumar) ) - 1Document6 pagesHelix Alliance - Resume (Dr. Appukutty Manickam (Kumar) ) - 1indo 5SNo ratings yet
- Maxillofacial Trauma With Head Injuries at A Tertiary Care Hospital in Chitwan, Nepal: Clinical, Medico-Legal, and Critical Care..Document9 pagesMaxillofacial Trauma With Head Injuries at A Tertiary Care Hospital in Chitwan, Nepal: Clinical, Medico-Legal, and Critical Care..Muhammad RizqiNo ratings yet
- Advances in The Local and Targeted Delivery of Anti-Infective Agents For Management of OsteomyelitisDocument20 pagesAdvances in The Local and Targeted Delivery of Anti-Infective Agents For Management of OsteomyelitisOtaam Ortopedia TraumatologíaNo ratings yet
- Negative Pressure Wound Therapy With Instillation in The Management of Infected And/or Chronic Wounds in Indian PatientsDocument9 pagesNegative Pressure Wound Therapy With Instillation in The Management of Infected And/or Chronic Wounds in Indian PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- JCM 11 06412 v2Document12 pagesJCM 11 06412 v2Ekin YamanNo ratings yet
- 2022 Article 795Document8 pages2022 Article 795Juan David Hernández CifuentesNo ratings yet
- International Emergency Nursing: A D A B CDocument9 pagesInternational Emergency Nursing: A D A B CPUSKESMAS KECAMATAN KEPULAUAN SERIBU UTARANo ratings yet
- Pharmaceutical Sciences: Incidence of Abdominal Trauma in A Tertiary Care HospitalDocument6 pagesPharmaceutical Sciences: Incidence of Abdominal Trauma in A Tertiary Care HospitaliajpsNo ratings yet
- Experts Advise Against Arthroscopy For Almost All Patients With Degenerative Knee Damage - FullDocument9 pagesExperts Advise Against Arthroscopy For Almost All Patients With Degenerative Knee Damage - FullWillbourNo ratings yet
- Comparative Assessment of Flap-Advancing TechniquesDocument9 pagesComparative Assessment of Flap-Advancing Techniques李潮忠No ratings yet
- Mosaicplasty For Symptomatic Articular Cartilage Defects of The Knee PDF 1899873866749381Document5 pagesMosaicplasty For Symptomatic Articular Cartilage Defects of The Knee PDF 1899873866749381JanetNo ratings yet
- (Journal of Neurosurgery - Spine) Risk Factors For Deep Surgical Site Infection Following Thoracolumbar Spinal SurgeryDocument10 pages(Journal of Neurosurgery - Spine) Risk Factors For Deep Surgical Site Infection Following Thoracolumbar Spinal SurgeryEugenia BocaNo ratings yet
- Validating The Brain Injury GuidelinesDocument9 pagesValidating The Brain Injury GuidelinesMarcus CezilloNo ratings yet
- Is Mechanism of Injury Alone A Useful Predictor of Major Trauma?Document7 pagesIs Mechanism of Injury Alone A Useful Predictor of Major Trauma?SulastriNo ratings yet
- International Journal of GerontologyDocument5 pagesInternational Journal of Gerontologydawn moonNo ratings yet
- Caso TeleconsultaDocument11 pagesCaso TeleconsultaNicolle CaroNo ratings yet
- JPM 11 00110Document12 pagesJPM 11 00110Johnny CshNo ratings yet
- 2) Neelakandan2014Document14 pages2) Neelakandan2014joteja8497No ratings yet
- Strategies to Prevent Surgical Site InfectionsDocument24 pagesStrategies to Prevent Surgical Site InfectionsCarissa SulaimanNo ratings yet
- Journal Pone 0255052Document14 pagesJournal Pone 0255052Saffa AzharaaniNo ratings yet
- DAIRDocument12 pagesDAIRCris JiménezNo ratings yet
- Prevention of Surgical Site Infections: Surgical Patient Care SeriesDocument11 pagesPrevention of Surgical Site Infections: Surgical Patient Care Seriestien duongNo ratings yet
- Design and Implementation of A Trauma Care BundleDocument7 pagesDesign and Implementation of A Trauma Care BundleNi Nyoman AstriningsihNo ratings yet
- 4 +Mustika+FatimahDocument8 pages4 +Mustika+FatimahEster DuwitNo ratings yet
- Trauma Cordon EspinalDocument11 pagesTrauma Cordon EspinalHeath HensleyNo ratings yet
- Role of Ultraviolet Disinfection in The Prevention of Surgical Site InfectionsDocument13 pagesRole of Ultraviolet Disinfection in The Prevention of Surgical Site InfectionsMohan DesaiNo ratings yet
- Trauma Pattern in A Level I East-European Trauma Center: July 2015Document5 pagesTrauma Pattern in A Level I East-European Trauma Center: July 2015Andreea SlabuNo ratings yet
- 2023 Complications and Treatment Errors in Peri-Implant Hard Tissue ManagementDocument22 pages2023 Complications and Treatment Errors in Peri-Implant Hard Tissue Managementmatias cofreNo ratings yet
- 1 s2.0 S0022346822002688 MainDocument8 pages1 s2.0 S0022346822002688 MaindrsubramanianNo ratings yet
- Management of Acute Spinal Cord Injury - A Summary of The Evidence Pertaining To The Acute Management, Operative and Non-Operative ManagementDocument12 pagesManagement of Acute Spinal Cord Injury - A Summary of The Evidence Pertaining To The Acute Management, Operative and Non-Operative Managementzee zeeNo ratings yet
- Trauma Systems Save Lives Is That EnoughDocument2 pagesTrauma Systems Save Lives Is That Enoughankur vermaNo ratings yet
- Optimising Prevention of Surgical Wound Complications: Detection, Diagnosis, Surveillance and PredictionDocument28 pagesOptimising Prevention of Surgical Wound Complications: Detection, Diagnosis, Surveillance and PredictionAngel PerezNo ratings yet
- Post Traumatic Endophthalmitis: Incidence and Risk FactorsDocument5 pagesPost Traumatic Endophthalmitis: Incidence and Risk FactorsIgnasius HansNo ratings yet
- Traumatic Brain Injury: Integrated Approaches To Improve Prevention, Clinical Care, and ResearchDocument63 pagesTraumatic Brain Injury: Integrated Approaches To Improve Prevention, Clinical Care, and Researchakish4uNo ratings yet
- Tieken CV 2023Document5 pagesTieken CV 2023api-568999633No ratings yet
- Pressure Ulcer Assessment and Treatment (PDFDrive)Document88 pagesPressure Ulcer Assessment and Treatment (PDFDrive)Amna AliNo ratings yet
- Epidemiology of Whiplash-Associated Disorders: F. Ioppolo and R. S. RizzoDocument5 pagesEpidemiology of Whiplash-Associated Disorders: F. Ioppolo and R. S. RizzoJeremi SetiawanNo ratings yet
- Rapid Recovery in Total Joint Arthroplasty: Contemporary StrategiesFrom EverandRapid Recovery in Total Joint Arthroplasty: Contemporary StrategiesNo ratings yet
- Physiology and Pathology of Physical and Psychological StressDocument60 pagesPhysiology and Pathology of Physical and Psychological StressBrunoNo ratings yet
- Prof - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenDocument40 pagesProf - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenBrunoNo ratings yet
- DR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianDocument36 pagesDR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianBruno100% (1)
- Hub and Spoke Model For STEMI Management - Tamil Nadu ModelDocument16 pagesHub and Spoke Model For STEMI Management - Tamil Nadu ModelBrunoNo ratings yet
- TAEI NTRI WorkshopDocument16 pagesTAEI NTRI WorkshopBrunoNo ratings yet
- Ms Ellaine Boo Role of Trauma NursingDocument35 pagesMs Ellaine Boo Role of Trauma NursingBrunoNo ratings yet
- DR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonDocument25 pagesDR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonBrunoNo ratings yet
- DR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsDocument32 pagesDR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsBruno100% (1)
- DR - Joseph Mathew: Trauma Units and Team WorkDocument39 pagesDR - Joseph Mathew: Trauma Units and Team WorkBrunoNo ratings yet
- Prof Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryDocument37 pagesProf Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryBrunoNo ratings yet
- Mrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNDocument11 pagesMrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNBrunoNo ratings yet
- DR - Ramana Rao Pre-Hospital Services in Tamil NaduDocument73 pagesDR - Ramana Rao Pre-Hospital Services in Tamil NaduBrunoNo ratings yet
- Prof DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareDocument46 pagesProf DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareBrunoNo ratings yet
- DR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemDocument29 pagesDR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemBrunoNo ratings yet
- Mr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusDocument25 pagesMr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusBruno100% (1)
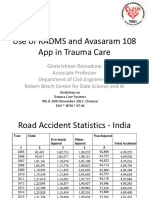
- Prof Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareDocument21 pagesProf Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareBrunoNo ratings yet
- Ian Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduDocument26 pagesIan Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduBrunoNo ratings yet
- DR - Darez Ahamed Vision For Tamil NaduDocument6 pagesDR - Darez Ahamed Vision For Tamil NaduBrunoNo ratings yet
- Neurosurgeon For A Social CauseDocument55 pagesNeurosurgeon For A Social CauseBrunoNo ratings yet
- How Tamil Nadu Eradicated Organ SaleDocument108 pagesHow Tamil Nadu Eradicated Organ SaleBrunoNo ratings yet
- TN Gazette 47 of 2013 Part VI Section 4Document84 pagesTN Gazette 47 of 2013 Part VI Section 4BrunoNo ratings yet
- Why Tamil Nadu Model Works Better in Eradicating Organ SaleDocument52 pagesWhy Tamil Nadu Model Works Better in Eradicating Organ SaleBrunoNo ratings yet
- Doctors' Role in Tackling Organ TradeDocument70 pagesDoctors' Role in Tackling Organ TradeBrunoNo ratings yet
- AR Rahman PDFDocument405 pagesAR Rahman PDFPitchai BalaNo ratings yet
- HMIS - Health Management Information System - Government of Tamil NaduDocument12 pagesHMIS - Health Management Information System - Government of Tamil NaduBruno100% (1)
- Nettle Rash Symptoms, Causes, TreatmentDocument2 pagesNettle Rash Symptoms, Causes, TreatmentArdave Laurente100% (1)
- Inspiration Powerpoint NoteDocument13 pagesInspiration Powerpoint Noteapi-201676767No ratings yet
- Section 5 - Students WorksheetDocument4 pagesSection 5 - Students WorksheetEsraa AhmedNo ratings yet
- Uganda Participatory Poverty Assessment Report 2000Document193 pagesUganda Participatory Poverty Assessment Report 2000FabioNo ratings yet
- Colposcopic Findings Prepubertal Assessed For Sexual Abuse: Genital GirlsDocument5 pagesColposcopic Findings Prepubertal Assessed For Sexual Abuse: Genital GirlsSusi PuspitaNo ratings yet
- Indian Herbs Cooking GuideDocument37 pagesIndian Herbs Cooking Guidehitesh mendirattaNo ratings yet
- AcupunctureDocument15 pagesAcupuncturezextorcNo ratings yet
- Pteridophytes MorphologyDocument79 pagesPteridophytes MorphologyBoopathiAyyanarMNo ratings yet
- Male infertility evaluation: what you need to knowDocument1 pageMale infertility evaluation: what you need to knowa jNo ratings yet
- 03 Biosecurity Jit PPT FinalDocument20 pages03 Biosecurity Jit PPT FinalReza WratsongkoNo ratings yet
- CPT Exam Study Guide: Health AssessmentsDocument3 pagesCPT Exam Study Guide: Health Assessmentssiriamma wiliamsNo ratings yet
- GEHC Brochure Senographe CareDocument7 pagesGEHC Brochure Senographe CareVremedSoluCionesNo ratings yet
- Mood Disorders - Bipolar Disorder: Professor Macdonald, MSN, RNDocument47 pagesMood Disorders - Bipolar Disorder: Professor Macdonald, MSN, RNmaha abdallahNo ratings yet
- Quantitative EstimationDocument4 pagesQuantitative EstimationSarah BODOFIANo ratings yet
- Kirit P. Mehta School of Law, Mumbai: A Project Submitted ONDocument12 pagesKirit P. Mehta School of Law, Mumbai: A Project Submitted ONNikit BaryaNo ratings yet
- MUSYAWARAH GURU MATA PELAJARAN BAHASA INGGRIS UJIAN SEKOLAHDocument13 pagesMUSYAWARAH GURU MATA PELAJARAN BAHASA INGGRIS UJIAN SEKOLAHASEP MALIKNo ratings yet
- 3rd Periodical Grade 10Document3 pages3rd Periodical Grade 10diomedescolar.13No ratings yet
- RT MapehDocument2 pagesRT MapehRowan ImperialNo ratings yet
- Internship Report JackDocument85 pagesInternship Report JackdamarismagererNo ratings yet
- Plant Based Diet A Way To Healthier Life: September 2020Document9 pagesPlant Based Diet A Way To Healthier Life: September 2020MihryazdNo ratings yet
- Envis Newsletter April 2014Document16 pagesEnvis Newsletter April 2014Mikel MillerNo ratings yet
- Common Medical Surgical MedicationsDocument36 pagesCommon Medical Surgical MedicationsAshley Etheredge100% (1)
- Fungi Classes ChartDocument1 pageFungi Classes ChartManav SinghNo ratings yet