You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- PDF Cerdas Bermedia Sosial CompressDocument2 pagesPDF Cerdas Bermedia Sosial CompressAlfiany SahrNo ratings yet
- Klasifikasi Nasal TraumaDocument4 pagesKlasifikasi Nasal TraumaAlfiany SahrNo ratings yet
- Prevention and Prognosis GigantismDocument1 pagePrevention and Prognosis GigantismAlfiany SahrNo ratings yet
- Laporan Skenario 1 Blok XX Semester 7Document12 pagesLaporan Skenario 1 Blok XX Semester 7Alfiany SahrNo ratings yet
- Patophysiology and Clinical Symptoms of Acidosis MetabolicDocument6 pagesPatophysiology and Clinical Symptoms of Acidosis MetabolicAlfiany SahrNo ratings yet
- CA MammaeDocument30 pagesCA MammaeAlfiany SahrNo ratings yet
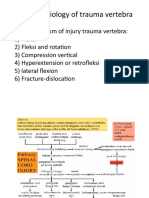
- Pathophysiology of Trauma VertebraDocument2 pagesPathophysiology of Trauma VertebraAlfiany SahrNo ratings yet
- Beginning of Management Head InjuryDocument2 pagesBeginning of Management Head InjuryAlfiany SahrNo ratings yet
- Pathophysiology of Trauma VertebraDocument2 pagesPathophysiology of Trauma VertebraAlfiany SahrNo ratings yet
- Pathophysiology of Trauma VertebraDocument2 pagesPathophysiology of Trauma VertebraAlfiany SahrNo ratings yet
- Pathophysiology of Trauma VertebraDocument2 pagesPathophysiology of Trauma VertebraAlfiany SahrNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- How To Identify Adhd ChildrenDocument6 pagesHow To Identify Adhd ChildrenKUNNAMPALLIL GEJO JOHNNo ratings yet
- Bed Bath Procedure: Presented By: Prof - Vijayreddy Vandali Dept of Medical-Surgical Nursing IndiaDocument17 pagesBed Bath Procedure: Presented By: Prof - Vijayreddy Vandali Dept of Medical-Surgical Nursing Indiaramzan aliNo ratings yet
- Guia de Interpretacion Resultados MicrobiologicosDocument19 pagesGuia de Interpretacion Resultados MicrobiologicosJuhaydith Hernandez AzuajeNo ratings yet
- AztreonamDocument2 pagesAztreonamHannahShaeHayesNo ratings yet
- COMMUNICATING EFFECTIVELYDocument34 pagesCOMMUNICATING EFFECTIVELYPallavi Modi100% (1)
- Abdominal AbscessDocument3 pagesAbdominal AbscessIchalAzNo ratings yet
- Culturally Competent Nursing CareDocument1 pageCulturally Competent Nursing CareYolanda WomackNo ratings yet
- Aldy Safruddin Rambe, Hasan Sjahrir, Moh Hasan MachfoedDocument4 pagesAldy Safruddin Rambe, Hasan Sjahrir, Moh Hasan MachfoedputrianabrsitompulNo ratings yet
- ENVOY DA Guding Catheter Brochure DSUS COD 0314 0017Document4 pagesENVOY DA Guding Catheter Brochure DSUS COD 0314 0017Tarun MathurNo ratings yet
- HCD Magazine 2014 VOL14Document70 pagesHCD Magazine 2014 VOL14hashim.mjNo ratings yet
- Neonatal Resuscitation Power PointDocument29 pagesNeonatal Resuscitation Power PointsameerarswNo ratings yet
- Dpope Nurs5327 Teachingphilosophy WebsiteDocument2 pagesDpope Nurs5327 Teachingphilosophy Websiteapi-496551085No ratings yet
- Parts of The Body and Health ProblemDocument13 pagesParts of The Body and Health ProblemSonia Tri AgustinaNo ratings yet
- International Code of Medical Ethics 2006Document2 pagesInternational Code of Medical Ethics 2006Kranthi ChirumamillaNo ratings yet
- National Safety Standards for HospitalsDocument51 pagesNational Safety Standards for HospitalsAyman Ali100% (4)
- Visit Report of DHQDocument2 pagesVisit Report of DHQUsman DastgirNo ratings yet
- NCP Impaired Urinary Elimination CRFDocument2 pagesNCP Impaired Urinary Elimination CRFNoel Cabamongan88% (8)
- Critical Soft-Tissue Dimensions With Dental Implantsand Treatment Concepts PDFDocument13 pagesCritical Soft-Tissue Dimensions With Dental Implantsand Treatment Concepts PDFgirl33No ratings yet
- Washing raw chicken increases risk of food poisoningDocument3 pagesWashing raw chicken increases risk of food poisoningsecretNo ratings yet
- Antipsychotics Mechanisms Indications SideEffectsDocument4 pagesAntipsychotics Mechanisms Indications SideEffectsRana MuhammadNo ratings yet
- 2020 What Is Arthritis 15 1Document32 pages2020 What Is Arthritis 15 1Oana BordeianuNo ratings yet
- Patient Satisfaction and Benefts of Music Therapy Services To Manage Stress and Pain in The Hospital Emergency DepartmentDocument25 pagesPatient Satisfaction and Benefts of Music Therapy Services To Manage Stress and Pain in The Hospital Emergency DepartmentBapak Sunaryo SPBU100% (1)
- Screem-Res Description 1Document4 pagesScreem-Res Description 1Jeanne Marie Vales100% (2)
- When All They Had Was LoveDocument14 pagesWhen All They Had Was LoveRahul Pinnamaneni100% (1)
- Transitional Care: DR - Vinoli.S.G Professor HOD Medical Surgical Nursing Dept Universal College of Nursing BangaloreDocument15 pagesTransitional Care: DR - Vinoli.S.G Professor HOD Medical Surgical Nursing Dept Universal College of Nursing BangalorevinoliNo ratings yet
- Ichthyosis Vulgaris: A Case Report and Review of LiteratureDocument3 pagesIchthyosis Vulgaris: A Case Report and Review of LiteratureJames Czar Fontanilla IlaganNo ratings yet
- Clinical Laboratory Techniques GuideDocument41 pagesClinical Laboratory Techniques GuideBalaji GandhiNo ratings yet
- Laporan Kasus Status EpileptikusDocument29 pagesLaporan Kasus Status EpileptikusPuji Yunisyah RahayuNo ratings yet
- Non Healing UlcersDocument36 pagesNon Healing UlcersIniya RajendranNo ratings yet
- Jurnal Farmakokinetik Dan Farmakodinamik Polimiksin BDocument11 pagesJurnal Farmakokinetik Dan Farmakodinamik Polimiksin BWildan Setyo RayandiNo ratings yet