You might also like
- Penatalaksanaan SyokDocument59 pagesPenatalaksanaan SyokArif NurfadhilahNo ratings yet
- Kul Sem 4 Heat Stroke N Fever UHT 2016Document63 pagesKul Sem 4 Heat Stroke N Fever UHT 2016NandaSuryaWijayaNo ratings yet
- Ophthalmology VisualsDocument28 pagesOphthalmology VisualsAditya Narayan100% (3)
- Nephrotic and Nephritic Syndrome: Med5010 LectureDocument65 pagesNephrotic and Nephritic Syndrome: Med5010 LectureFreeburn Simunchembu100% (1)
- Nephrotic Syndrome 2016Document45 pagesNephrotic Syndrome 2016alaaNo ratings yet
- Fluids and Electrolyte PediatricsDocument41 pagesFluids and Electrolyte PediatricsYusron BishryNo ratings yet
- Cme Acs 2. Stemi (Izzah)Document36 pagesCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiNo ratings yet
- MiokarditisDocument30 pagesMiokarditismaulana wasis0% (1)
- Clinical Evaluation of DehydrationDocument5 pagesClinical Evaluation of DehydrationEricka Lyn Arenas MonzonNo ratings yet
- Askep MCI - AchirmanDocument53 pagesAskep MCI - AchirmanmarthaNo ratings yet
- Tachyarrhythmia SDocument46 pagesTachyarrhythmia SAsif HameedNo ratings yet
- Hepatorenal SyndromeDocument6 pagesHepatorenal SyndromeEveline YNo ratings yet
- Gangguan Keseimbangan Cairan Dan ElektrolitDocument77 pagesGangguan Keseimbangan Cairan Dan ElektrolitPutri Santri100% (2)
- Death Case Dr. MeikoDocument49 pagesDeath Case Dr. MeikoMohamad ZulfikarNo ratings yet
- FIXED PPT Case Report EsterDocument39 pagesFIXED PPT Case Report Esterririn esterinaNo ratings yet
- PATHOPHYSIOLOGY OF SHOCKDocument56 pagesPATHOPHYSIOLOGY OF SHOCKDr. Haricharan ANo ratings yet
- Ringer Asetat Pada AnakDocument72 pagesRinger Asetat Pada Anaknanda surastyo100% (1)
- Resources - Fat Embolism Syndrome (FES)Document19 pagesResources - Fat Embolism Syndrome (FES)Hareen Reddy100% (1)
- Critical CareDocument8 pagesCritical Careapi-280066855No ratings yet
- 5e69b4ff83ed0-Fluid Responsiveness, Dynamic and Static Hemodynamic MonitoringDocument28 pages5e69b4ff83ed0-Fluid Responsiveness, Dynamic and Static Hemodynamic Monitoringyulya100% (1)
- Rheumatic Fever: DR: Kaem Shir AliDocument24 pagesRheumatic Fever: DR: Kaem Shir AliMwanja Moses100% (1)
- SepsisDocument33 pagesSepsisv_vijayakanth7656No ratings yet
- Preoperative Assessment ChecklistDocument27 pagesPreoperative Assessment ChecklistHairina MazlanNo ratings yet
- Recent Update in The Management of Invasive Fungal InfectionDocument30 pagesRecent Update in The Management of Invasive Fungal Infectionanoop61100% (2)
- Fluid N Electrolyte BalanceDocument60 pagesFluid N Electrolyte BalanceAnusha Verghese67% (3)
- Surgically Correctable Causes of Secondary HypertensionDocument29 pagesSurgically Correctable Causes of Secondary HypertensionVibha Gupta100% (4)
- Iron Deficiency Anemia GuideDocument54 pagesIron Deficiency Anemia GuideRamsha ZafarNo ratings yet
- Nephrotic SyndromeDocument24 pagesNephrotic SyndromeJawad SaleemNo ratings yet
- Clinical Approach to HypertensionDocument16 pagesClinical Approach to HypertensionShradha KhuranaNo ratings yet
- HHS Guide to Hypertensive Heart DiseaseDocument27 pagesHHS Guide to Hypertensive Heart DiseaseEvi MiwaNo ratings yet
- Surfactant PresentationDocument18 pagesSurfactant PresentationMaadaNo ratings yet
- Potassium ParticipantsDocument21 pagesPotassium ParticipantsSkylar IvyNo ratings yet
- Pedal EdemaDocument5 pagesPedal EdemaPunyashlok BiswalNo ratings yet
- ESRDDocument10 pagesESRDKayle Irah CaburnayNo ratings yet
- Dyslipidemia Update by DR SarmaDocument96 pagesDyslipidemia Update by DR SarmaDewi NofiantiNo ratings yet
- Sirosis HatiDocument10 pagesSirosis HatisakinahNo ratings yet
- TLS FinalDocument69 pagesTLS FinalGrace Arthur100% (1)
- Interpretasi ElektrokardiografiDocument60 pagesInterpretasi ElektrokardiografiYogi GustriansyahNo ratings yet
- Nephrotic SyndromeDocument12 pagesNephrotic Syndromewidya_fk08No ratings yet
- Restrictive Lung DiseaseDocument32 pagesRestrictive Lung DiseaseSalman Khan100% (1)
- The Complications of DiabetesDocument1 pageThe Complications of DiabetesMiguel Cuevas DolotNo ratings yet
- Vitamin D Deficiency: Epidemiology, Pathophysiology and ManagementDocument61 pagesVitamin D Deficiency: Epidemiology, Pathophysiology and ManagementSalmanNo ratings yet
- COPD: Chronic Obstructive Pulmonary Disease ExplainedDocument52 pagesCOPD: Chronic Obstructive Pulmonary Disease ExplainedErik II100% (1)
- CURRICULUM VITAE OF DENGUE EXPERTDocument59 pagesCURRICULUM VITAE OF DENGUE EXPERTsaladass 2No ratings yet
- FLUID AND ELECTROLYTE THERAPYDocument47 pagesFLUID AND ELECTROLYTE THERAPYSeblewongel AsemeNo ratings yet
- PneumothoraxDocument26 pagesPneumothoraxToni-Ann AllenNo ratings yet
- Anatomi Dan Fisiologi PerkemihanDocument89 pagesAnatomi Dan Fisiologi Perkemihannia djNo ratings yet
- Farmakologi KlinikDocument20 pagesFarmakologi KlinikNovasuryati100% (1)
- Congenital Adrenal HyperplasiaDocument14 pagesCongenital Adrenal HyperplasiabangkitayuNo ratings yet
- Tocolytic Agents and Anticonvulsants for Preterm LabourDocument95 pagesTocolytic Agents and Anticonvulsants for Preterm LabourPriya jNo ratings yet
- Perioperative Management in Diabetes MellitusDocument20 pagesPerioperative Management in Diabetes MellitusChristopher RyalinoNo ratings yet
- NN Jaundice - MoteeDocument70 pagesNN Jaundice - MoteeMhmNo ratings yet
- Arthritis, Suppurative Arthritis) : Pyogenic Arthritis (Septic Arthritis, InfectiveDocument4 pagesArthritis, Suppurative Arthritis) : Pyogenic Arthritis (Septic Arthritis, InfectiveRajveerNo ratings yet
- Understanding Corpulmonale: Causes, Symptoms and TreatmentDocument17 pagesUnderstanding Corpulmonale: Causes, Symptoms and TreatmentSurya ArhNo ratings yet
- MediastinumDocument27 pagesMediastinumAndrei PanaNo ratings yet
- Daftar Nutrisi ParenteralDocument6 pagesDaftar Nutrisi Parenteralcitrahdyn100% (1)
- Clinical Reasoning For Nursing Students - Glossary of TermsDocument22 pagesClinical Reasoning For Nursing Students - Glossary of Termsmillstoneridge1100% (1)
- Approach To FeverDocument80 pagesApproach To FeverRaditia AbrahamNo ratings yet
- Managing Hypertensive CrisesDocument31 pagesManaging Hypertensive CrisesAmanda DavisNo ratings yet
- Hipertensi EmergencyDocument31 pagesHipertensi Emergencyintan trimauliaNo ratings yet
- FIX Leg UlcerDocument59 pagesFIX Leg UlcerDekka Andra100% (2)
- Cardiovascular Clinical ExaminationDocument27 pagesCardiovascular Clinical ExaminationAshiniNo ratings yet
- Thromboembolic DisordersDocument11 pagesThromboembolic Disordersannu panchalNo ratings yet
- Blood ComponentsDocument2 pagesBlood ComponentsParul ShahNo ratings yet
- Systolic MurmursDocument10 pagesSystolic MurmursRizqan Fahlevvi AkbarNo ratings yet
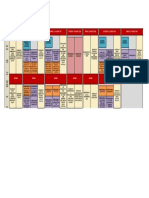
- Program at Glance WECOC 2021-Updated Juli 2021Document1 pageProgram at Glance WECOC 2021-Updated Juli 2021Bambang SupriadiNo ratings yet
- Blood Supply of The Brain - ModifiedDocument24 pagesBlood Supply of The Brain - ModifiedSamo BeainoNo ratings yet
- Myocardial Infarction Risk FactorsDocument4 pagesMyocardial Infarction Risk FactorsMark Emil BautistaNo ratings yet
- Cardiovascular Diseases Burden in BrazilDocument82 pagesCardiovascular Diseases Burden in Brazilpcpainel smfNo ratings yet
- Laporan Kasus VSDDocument40 pagesLaporan Kasus VSDShirin LaleNo ratings yet
- Nicardipine DripDocument8 pagesNicardipine DripRichard Ines ValinoNo ratings yet
- The Romanian Society of Cardiology BoardDocument4 pagesThe Romanian Society of Cardiology Boardmyreille_mNo ratings yet
- INFLAMMATION: A Protective Response to InjuryDocument22 pagesINFLAMMATION: A Protective Response to InjuryRamesh KumarNo ratings yet
- IABP Learning PackageDocument35 pagesIABP Learning Packagekingjoon 78100% (1)
- Final Exam Paper Provides InstructionsDocument35 pagesFinal Exam Paper Provides InstructionsAndreea AndraNo ratings yet
- Blood Vessel and Lymphatic Lab OutputDocument12 pagesBlood Vessel and Lymphatic Lab OutputDayledaniel SorvetoNo ratings yet
- Valsartan in The Treatment of Hypertension: OriginalDocument4 pagesValsartan in The Treatment of Hypertension: Originaldini hanifaNo ratings yet
- CVADocument11 pagesCVACla100% (4)
- AAA Screening - Spanos 2017Document3 pagesAAA Screening - Spanos 2017Vlad NeagoeNo ratings yet
- 1st Year PhysiologyDocument15 pages1st Year PhysiologyMaheen AnwaarNo ratings yet
- Sample of Clinical PortraitDocument3 pagesSample of Clinical PortraitSweetie StarNo ratings yet
- Critical Care NotesDocument18 pagesCritical Care NotesjulieNo ratings yet
- 2 - PPT DR Erika Maharani SPJPDocument42 pages2 - PPT DR Erika Maharani SPJPAmry YusufNo ratings yet
- Cardiostudy 2Document2 pagesCardiostudy 2Anita CheramieNo ratings yet
- Drug Study: Valerie V. Villanueva BN3-CDocument2 pagesDrug Study: Valerie V. Villanueva BN3-CA.No ratings yet
- Amat Ncma 219 CT 2 BTDocument4 pagesAmat Ncma 219 CT 2 BTRaf AmatNo ratings yet
- Key Questions in Cardiac SurgeryDocument522 pagesKey Questions in Cardiac SurgeryRenan Petinelli100% (3)
- Valvular Heart DiseaseDocument27 pagesValvular Heart DiseaseOwen J. WieseNo ratings yet
- Improving Knowledge on Hypertension PreventionDocument9 pagesImproving Knowledge on Hypertension PreventionIntan OktavianiNo ratings yet
- Arrows Consele PDFDocument221 pagesArrows Consele PDFIsai Lara OsoriaNo ratings yet