You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Odontogenic Cysts and Tumors GuideDocument41 pagesOdontogenic Cysts and Tumors GuideSeca mandiNo ratings yet
- Effect of Cervical Margin Relocation on Marginal Quality of CAD/CAM CrownsDocument8 pagesEffect of Cervical Margin Relocation on Marginal Quality of CAD/CAM CrownsIvy MedNo ratings yet
- Effects of Maxillary Protraction For Early Correction of Class IIIDocument7 pagesEffects of Maxillary Protraction For Early Correction of Class IIIMariana SantosNo ratings yet
- Review of Space Maintainers for Preventing MalocclusionDocument5 pagesReview of Space Maintainers for Preventing MalocclusionHabeeb AL-AbsiNo ratings yet
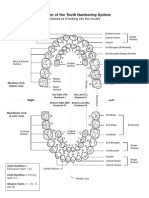
- Diagram of The Tooth Numbering SystemDocument1 pageDiagram of The Tooth Numbering Systemsaleh900No ratings yet
- Periodontal LigamentDocument38 pagesPeriodontal LigamentyogeshNo ratings yet
- Self-Perception of Periodontal Health and Associated Factors: A Cross-Sectional Population-Based StudyDocument14 pagesSelf-Perception of Periodontal Health and Associated Factors: A Cross-Sectional Population-Based StudyatikramadhaniNo ratings yet
- Indirect Retainers: Chapter OutlineDocument5 pagesIndirect Retainers: Chapter OutlineRizki Dwi LestariNo ratings yet
- Case Presentation: Done By: Dr. Hanan Abu MnaizelDocument60 pagesCase Presentation: Done By: Dr. Hanan Abu Mnaizelaung NaingmyoNo ratings yet
- Art and Science of Operative DentistryDocument699 pagesArt and Science of Operative DentistryPatricia Popescu100% (3)
- Case SheetDocument4 pagesCase SheetFatimah AmjedNo ratings yet
- Lingual Orthodontics - A Review: Invited ArticlesDocument8 pagesLingual Orthodontics - A Review: Invited ArticlesHARITHA H.PNo ratings yet
- 9205 PDFDocument10 pages9205 PDFAlexandraNo ratings yet
- Denture DuplicationDocument70 pagesDenture DuplicationMuhammad Riaz KhanNo ratings yet
- Ijerph 20 04481 v2 PDFDocument29 pagesIjerph 20 04481 v2 PDFNguyen Hong AnNo ratings yet
- Vertical Root Fracture !Document42 pagesVertical Root Fracture !Dr Dithy kkNo ratings yet
- ORTHODONTICS CLASSIFICATION REVISITEDDocument7 pagesORTHODONTICS CLASSIFICATION REVISITEDDharampal SinghNo ratings yet
- Seminar Presentation On Enamel: By-Devanshi Sharma P.G.1 Year Dept. of Cons. Dentistry & EndoDocument105 pagesSeminar Presentation On Enamel: By-Devanshi Sharma P.G.1 Year Dept. of Cons. Dentistry & EndoDevanshi SharmaNo ratings yet
- Dental 2Document8 pagesDental 2Jerwin Sarcia RemocalNo ratings yet
- HealthDocument16 pagesHealthMaria Lucille Mejias IINo ratings yet
- Condiciones ParticularesDocument19 pagesCondiciones ParticularesBlaise BowlyNo ratings yet
- Placa de Acetato BioartDocument5 pagesPlaca de Acetato BioartlenzajrNo ratings yet
- The Obsolescence of Formocresol: B. LewisDocument4 pagesThe Obsolescence of Formocresol: B. LewisAlan Vargas100% (1)
- Complete Denture Treatment With A Flat Ridge Using Semi-Adjustable ArticulatorDocument5 pagesComplete Denture Treatment With A Flat Ridge Using Semi-Adjustable ArticulatorDiny Ilmy AfifahNo ratings yet
- Concept: Captek™ Are Crowns and Bridges That Mimic and Surpass Natural Teeth in Esthetic and FunctionDocument50 pagesConcept: Captek™ Are Crowns and Bridges That Mimic and Surpass Natural Teeth in Esthetic and FunctionPolet Aline Sánchez SosaNo ratings yet
- Sectional Matrix: Step-By-Step Directions For Their Clinical UseDocument5 pagesSectional Matrix: Step-By-Step Directions For Their Clinical UseRaniyah Az-zahraNo ratings yet
- Non-Surgical Pocket Therapy Dental OclusionDocument14 pagesNon-Surgical Pocket Therapy Dental OclusionFelipe Ulloa CastilloNo ratings yet
- Pi Is 0889540615013311Document5 pagesPi Is 0889540615013311msoaresmirandaNo ratings yet
- Pulp and Periapical DiseasesDocument127 pagesPulp and Periapical DiseasesJitender Reddy75% (4)
- CBL in EnglishDocument8 pagesCBL in EnglishPutri MayangNo ratings yet