You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- List of SpecialistsDocument2 pagesList of SpecialistsiwennieNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Mcqs Inflammatory Bowel DiseaseDocument2 pagesMcqs Inflammatory Bowel Diseaseiwennie100% (1)
- Guide To Medical Standards of Fitness To DriveDocument53 pagesGuide To Medical Standards of Fitness To DriveiwennieNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Osce Ear Nose N Telinga. P Throat!-From Siti Zarina. MueheheDocument43 pagesOsce Ear Nose N Telinga. P Throat!-From Siti Zarina. MueheheiwennieNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Xraysinent 170104125612Document30 pagesXraysinent 170104125612iwennieNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Ivanaesthetics 160916154203Document70 pagesIvanaesthetics 160916154203iwennieNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Weight-for-Height GIRLS: 2 To 5 Years (Z-Scores)Document1 pageWeight-for-Height GIRLS: 2 To 5 Years (Z-Scores)Malisa LukmanNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Menstrual CycleDocument6 pagesThe Menstrual CycleiwennieNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Miscarriage Early Pregnancy LossDocument10 pagesMiscarriage Early Pregnancy LossiwennieNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Common Complications of PregnancyDocument34 pagesCommon Complications of PregnancyiwennieNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- How To Read A CTGDocument11 pagesHow To Read A CTGiwennieNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Blood DyscrasiaDocument136 pagesBlood DyscrasiaiwennieNo ratings yet
- Physiological Aspects of Normal PregnancyDocument4 pagesPhysiological Aspects of Normal PregnancyiwennieNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- BR J Hosp Med The Babinski SignDocument8 pagesBR J Hosp Med The Babinski SigniwennieNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 3 Minute Exam of ChildrenDocument2 pages3 Minute Exam of ChildreniwennieNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Dimitris Loukopoulos PDFDocument46 pagesDimitris Loukopoulos PDFiwennieNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- IntroductionDocument33 pagesIntroductioniwennieNo ratings yet
- Exercise Fluids Topic 1 PDFDocument2 pagesExercise Fluids Topic 1 PDFiwennieNo ratings yet
- Complication of TBDocument15 pagesComplication of TBTintin PoncianoNo ratings yet
- المعدلات الطبيعية لمعظم الاختبارت بالمختبرDocument4 pagesالمعدلات الطبيعية لمعظم الاختبارت بالمختبرMohamedErrmaliNo ratings yet
- Substance Use and Abuse Among AdolescentsDocument9 pagesSubstance Use and Abuse Among AdolescentsiwennieNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Complication of TBDocument15 pagesComplication of TBTintin PoncianoNo ratings yet
- Pediatric Heart Failure 2015Document7 pagesPediatric Heart Failure 2015iwennieNo ratings yet
- Sterilization and DisinfectionDocument3 pagesSterilization and DisinfectionAthul GurudasNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Osteomalacia and RicketsDocument4 pagesOsteomalacia and RicketsiwennieNo ratings yet
- Adolescent and YouthDocument2 pagesAdolescent and YouthiwennieNo ratings yet
- Pathology: Dr. Muriithi: 2 Year: 1 SemesterDocument2 pagesPathology: Dr. Muriithi: 2 Year: 1 SemesteriwennieNo ratings yet
- Aneamis and HaematologyDocument129 pagesAneamis and HaematologyiwennieNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Parasympathetic Vs Sympathetic Nervous System - Difference and ComparisonDocument4 pagesParasympathetic Vs Sympathetic Nervous System - Difference and ComparisoniwennieNo ratings yet
- Express™ XT - VPS Impression MaterialsDocument6 pagesExpress™ XT - VPS Impression Materials3mEgyptCoordinatorNo ratings yet
- Normal GFR in ChildDocument8 pagesNormal GFR in ChildbobbypambudimdNo ratings yet
- Gregory Classification, and These Two Classifications Will Give UsDocument15 pagesGregory Classification, and These Two Classifications Will Give Usapi-19840404No ratings yet
- Module 2Document2 pagesModule 2Duchess Juliane Jose MirambelNo ratings yet
- Richard Belli WorkshopDocument62 pagesRichard Belli WorkshopalicefreespiritNo ratings yet
- AdenoidsDocument8 pagesAdenoidsUjjawalShriwastavNo ratings yet
- Couple Therapy Clinician Guide For Partners With DepressionDocument28 pagesCouple Therapy Clinician Guide For Partners With Depressionelias_reyes100% (1)
- MCEM Toxicology MCQDocument110 pagesMCEM Toxicology MCQAnkita Sinha100% (4)
- Ham D PDFDocument1 pageHam D PDFRabiatul AdawiyahNo ratings yet
- He MaDocument25 pagesHe MaBeep TerradoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- AustAlctreatguidelines 2009 PDFDocument255 pagesAustAlctreatguidelines 2009 PDFFrizam DwindamuldanNo ratings yet
- Filaria PPT - ClassDocument59 pagesFilaria PPT - ClassGauravMeratwal100% (2)
- Ahead Adc MCQDocument12 pagesAhead Adc MCQSOMVIR KUMARNo ratings yet
- ParacetamolDocument24 pagesParacetamolFriné MirandaNo ratings yet
- About Arteriovenous Overview!!!Document7 pagesAbout Arteriovenous Overview!!!Cj UritaNo ratings yet
- Calder 2016 - Meta Analysis and Suggested Guidelines For Prevention of Venous Thromboembolism (VTE) in Foot and Ankle SurgeryDocument12 pagesCalder 2016 - Meta Analysis and Suggested Guidelines For Prevention of Venous Thromboembolism (VTE) in Foot and Ankle SurgeryNoel Yongshen LeeNo ratings yet
- Complications of Peptic Ulcer Disease: Surgical ManagementDocument57 pagesComplications of Peptic Ulcer Disease: Surgical ManagementJoan LuisNo ratings yet
- Classification of ArticulatorsDocument4 pagesClassification of ArticulatorsRishiraj Jaiswal67% (3)
- DCFS Mandated FormDocument1 pageDCFS Mandated FormAshraf AhmedNo ratings yet
- Ambulatory Surgical CareDocument265 pagesAmbulatory Surgical CareThamizhanban R100% (2)
- The Effects of Qigong On Reducing Stress and Anxiety and Enhancing Body Mind Well BeingDocument10 pagesThe Effects of Qigong On Reducing Stress and Anxiety and Enhancing Body Mind Well BeingSamo JaNo ratings yet
- 666 CDR - Scale PDFDocument10 pages666 CDR - Scale PDFIkanpaus Di BlogspotNo ratings yet
- Anaemia in PregnancyDocument15 pagesAnaemia in PregnancyNorshahidah Ieda100% (1)
- Reflection Paper Raul BallesterosDocument1 pageReflection Paper Raul BallesterosJay-ar Jay-arNo ratings yet
- MOH Regulations For EAS & MTS (PAOs)Document13 pagesMOH Regulations For EAS & MTS (PAOs)T33MOTEE90No ratings yet
- Free From Harm Final Report ResumenDocument4 pagesFree From Harm Final Report ResumenMiguel Armando Zúñiga OlivaresNo ratings yet
- VM in BpocDocument19 pagesVM in BpocAndreea Livia DumitrescuNo ratings yet
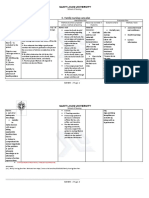
- C. Family Nursing Care Plan: Saint Louis UniversityDocument2 pagesC. Family Nursing Care Plan: Saint Louis UniversityLEONELLGABRIEL RAGUINDIN0% (1)
- Asthma Nursing Care Plans - LippincottDocument45 pagesAsthma Nursing Care Plans - LippincottDyllanoNo ratings yet
- Erb's PalsyDocument18 pagesErb's PalsyMegha PataniNo ratings yet
- The Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanFrom EverandThe Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanRating: 4.5 out of 5 stars4.5/5 (12)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- Mama Might Be Better Off Dead: The Failure of Health Care in Urban AmericaFrom EverandMama Might Be Better Off Dead: The Failure of Health Care in Urban AmericaNo ratings yet
- Epic Measures: One Doctor. Seven Billion Patients.From EverandEpic Measures: One Doctor. Seven Billion Patients.Rating: 4 out of 5 stars4/5 (13)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceFrom EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceRating: 4.5 out of 5 stars4.5/5 (11)