You might also like
- Child Psychopathology: Child Psychopathology Is The Manifestation of Psychological Disorders in Children andDocument7 pagesChild Psychopathology: Child Psychopathology Is The Manifestation of Psychological Disorders in Children andMarvellous MunhuwaNo ratings yet
- Psychological AdjustmentDocument100 pagesPsychological AdjustmentRagil Adist Surya PutraNo ratings yet
- UW Allergy + Immuno - Educational Objectives PDFDocument25 pagesUW Allergy + Immuno - Educational Objectives PDFDrbee10No ratings yet
- Yoga and PainDocument29 pagesYoga and PainGanesh Babu100% (1)
- Problems Related To Abuse or NeglectDocument25 pagesProblems Related To Abuse or Neglectapi-3797941100% (5)
- Schistosomiasis Case StudyDocument5 pagesSchistosomiasis Case Studyapi-318749549No ratings yet
- Action Plan For ClinicDocument2 pagesAction Plan For ClinicMelanie Delos Santos100% (3)
- Obsessive Compulsive Disorder: Patient Treatment ManualDocument20 pagesObsessive Compulsive Disorder: Patient Treatment ManualJay DraperNo ratings yet
- PathophysiologyDocument4 pagesPathophysiologyAngelou Joefred Congreso100% (1)
- Pathophysiology Septic ShockDocument26 pagesPathophysiology Septic ShockTinea Sycillia100% (1)
- Abruptio PlacentaDocument8 pagesAbruptio PlacentaNutz TolentinoNo ratings yet
- Pathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsDocument2 pagesPathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsAb Staholic Boii100% (1)
- Contact DermatitisDocument70 pagesContact DermatitisThariq Mubaraq DrcNo ratings yet
- 7-Steps For DI Systematic ApproachDocument8 pages7-Steps For DI Systematic ApproachDrDeepak Pawar71% (7)
- (FCM) 1.1 Tools in Family AssesmentDocument7 pages(FCM) 1.1 Tools in Family AssesmentAC BCNo ratings yet
- Upper Gastrointestinal Bleeding (Ugib) : First Shift: August 13, 2018Document10 pagesUpper Gastrointestinal Bleeding (Ugib) : First Shift: August 13, 2018Angelo Dela Cruz VillaromanNo ratings yet
- Benefits Summary PhilippinesDocument2 pagesBenefits Summary PhilippinesRose GeeNo ratings yet
- Answer and Rationale Psychiatric NursingDocument23 pagesAnswer and Rationale Psychiatric NursingCharles Gerard B. BeluanNo ratings yet
- Fatima Alatas - Approach of Cholestatic JaundiceDocument35 pagesFatima Alatas - Approach of Cholestatic JaundiceEnny AndrianiNo ratings yet
- Anestesi Obat ObatanDocument72 pagesAnestesi Obat ObatanfujiNo ratings yet
- GASTROSCHISISDocument4 pagesGASTROSCHISISVin Custodio100% (1)
- Φ PathophysiologyDocument4 pagesΦ PathophysiologyMariah AshooriyanNo ratings yet
- Nursing Care Plan General Objective: To Promote Safety Through Prevention of The Spread of InfectionDocument3 pagesNursing Care Plan General Objective: To Promote Safety Through Prevention of The Spread of InfectionitsmeayaNo ratings yet
- Case 6: Delos Reyes, Lasac, Majid, Mamangun, YuDocument49 pagesCase 6: Delos Reyes, Lasac, Majid, Mamangun, YuAbdullah Bin MajidNo ratings yet
- Rheumatic Heart DiseaseDocument3 pagesRheumatic Heart DiseaseDee SarajanNo ratings yet
- 6 Kuliah Liver CirrhosisDocument55 pages6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- Mechanism of HypertensionDocument4 pagesMechanism of HypertensionAlya Putri KhairaniNo ratings yet
- Initial PE and Labs History Initial Impression: Location &Document1 pageInitial PE and Labs History Initial Impression: Location &kaydee.arNo ratings yet
- Case Stude NNJDocument6 pagesCase Stude NNJmuzamirNo ratings yet
- My Pediatric Rotation ReflectionsDocument4 pagesMy Pediatric Rotation ReflectionsAdepoju Victor AbiolaNo ratings yet
- II. PATHOPHYSIOLOGY (Schematic Diagram) : Risk Factors Predisposing FactorsDocument2 pagesII. PATHOPHYSIOLOGY (Schematic Diagram) : Risk Factors Predisposing FactorseeymeeNo ratings yet
- Pa Tho Physiology of RaDocument7 pagesPa Tho Physiology of Ralisalmar2008No ratings yet
- Acute Rheumatic Fever PathophysiologyDocument1 pageAcute Rheumatic Fever PathophysiologyMoonyeen Jann Casera BalicNo ratings yet
- Dermoid CystDocument29 pagesDermoid CystAlik ChuaNo ratings yet
- Portal Vein Thrombus ChildrenDocument11 pagesPortal Vein Thrombus ChildrenViswas ChhapolaNo ratings yet
- Schematic Diagram MyomaDocument2 pagesSchematic Diagram MyomaJandz MN100% (2)
- SAMDocument108 pagesSAMAlimyon Abilar MontoloNo ratings yet
- 1 LiverDocument10 pages1 LiverAlbino Fulgencio Santos III100% (1)
- Pathophysiology of Tetanus: Precipitating Factors: Predisposing FactorsDocument2 pagesPathophysiology of Tetanus: Precipitating Factors: Predisposing FactorsPernel Jose Alam Micubo100% (1)
- Epidemiology, Pathogenesis, and Pathology of NeuroblastomaDocument21 pagesEpidemiology, Pathogenesis, and Pathology of NeuroblastomaHandre PutraNo ratings yet
- Communicable Disease ChartDocument1 pageCommunicable Disease ChartArlan AbraganNo ratings yet
- Case - LeptospirosisDocument39 pagesCase - LeptospirosisKimm Delos ReyesNo ratings yet
- Hirschsprung's DiseaseDocument18 pagesHirschsprung's DiseaseanisyahNo ratings yet
- Typhoid FeverDocument30 pagesTyphoid FeversakuarNo ratings yet
- Renal Concept MapDocument8 pagesRenal Concept MapXtine CajiNo ratings yet
- Idiophatic Thrombocytopenic Purpura (ITP) in PregnancyDocument27 pagesIdiophatic Thrombocytopenic Purpura (ITP) in PregnancyAdietya Bima PrakasaNo ratings yet
- Obstructive Jaundice and Perioperative ManagementsDocument8 pagesObstructive Jaundice and Perioperative ManagementsTri UtomoNo ratings yet
- Schistosomiasis (From Anatomy To Pathophysiology)Document10 pagesSchistosomiasis (From Anatomy To Pathophysiology)Tiger Knee100% (1)
- Hydatidiform Mole: PGI Sia, Kevin PGI Tan, SheilaDocument80 pagesHydatidiform Mole: PGI Sia, Kevin PGI Tan, SheilaSheila Mary TanNo ratings yet
- Case Presentation of Acute PyelonephritisDocument1 pageCase Presentation of Acute PyelonephritisANALYN ANUBNo ratings yet
- Cues Problem Physiologic Behavioral: Date Identified: July 19, 2016 Subjective CuesDocument2 pagesCues Problem Physiologic Behavioral: Date Identified: July 19, 2016 Subjective CuesitsmeayaNo ratings yet
- DIC Case StudyDocument7 pagesDIC Case StudyRobertNo ratings yet
- 55 61 Brain AbscessDocument7 pages55 61 Brain AbscessNadia OktarinaNo ratings yet
- Chronic PyelonephritisDocument5 pagesChronic PyelonephritisIsak ShatikaNo ratings yet
- Ov Ov OvDocument15 pagesOv Ov OvHayyana Mae Taguba LadiaNo ratings yet
- EAMC DFCM OPD Charting Guidelines As of March 2022Document19 pagesEAMC DFCM OPD Charting Guidelines As of March 2022Adrian MaterumNo ratings yet
- Small Bowel ObstructionDocument2 pagesSmall Bowel ObstructionSrividya PushpalaNo ratings yet
- Pediatrics: 2 Case ReportDocument50 pagesPediatrics: 2 Case ReportSam Raven AndresNo ratings yet
- Abnormal Uterine BleedingDocument2 pagesAbnormal Uterine BleedingNatasha EnidNo ratings yet
- Nursing Case Study HirschsprungsDocument7 pagesNursing Case Study HirschsprungsEdilyn BalicaoNo ratings yet
- CHAPTER 24 Williams OBDocument3 pagesCHAPTER 24 Williams OBJulienne Sanchez-Salazar100% (2)
- Poststreptococcal Glomerulonephritis - UpToDateDocument21 pagesPoststreptococcal Glomerulonephritis - UpToDateHandre Putra100% (1)
- Case Study #5Document2 pagesCase Study #5Jenny Jenders100% (1)
- Renal Concept MapDocument8 pagesRenal Concept MapRob DavilaNo ratings yet
- PathophysiologyDocument5 pagesPathophysiologyJessyl GirayNo ratings yet
- Case Presentation Scripts For Morning Meeting 1Document3 pagesCase Presentation Scripts For Morning Meeting 1Jam Knows RightNo ratings yet
- Live Preterm Baby Delivered NSDDocument13 pagesLive Preterm Baby Delivered NSDKristine Anne SorianoNo ratings yet
- Oncology Nursing Part 1 2Document51 pagesOncology Nursing Part 1 2fleur harrisonNo ratings yet
- Immune Thrombocytopenic Purpura 1 Immune Pathophysiology of Primary Immune ThrombocytopeniaDocument6 pagesImmune Thrombocytopenic Purpura 1 Immune Pathophysiology of Primary Immune ThrombocytopeniaMikeyNo ratings yet
- First Aid Step 1 2017 Sample RevisionsDocument9 pagesFirst Aid Step 1 2017 Sample RevisionsFirst Aid/USMLE-Rx100% (2)
- ITAT Holds That Charitable Trust Running Max Hospital Was Charitable To Only To Corporate Max Group of Companies and Uncharitable' Towards The Society or PublicDocument46 pagesITAT Holds That Charitable Trust Running Max Hospital Was Charitable To Only To Corporate Max Group of Companies and Uncharitable' Towards The Society or PublicLive LawNo ratings yet
- Patient Profile Data Form: Advance DirectivesDocument6 pagesPatient Profile Data Form: Advance DirectivesMa Cecilia SorianoNo ratings yet
- Soyabean Milk ReportDocument10 pagesSoyabean Milk Reportprakhalgoyal100% (1)
- Scio and Its Functionality and UsesDocument5 pagesScio and Its Functionality and UsesAndy MilitaruNo ratings yet
- Perineal RuptureDocument24 pagesPerineal RuptureIzz ShuhaimiNo ratings yet
- Vitamin EDocument11 pagesVitamin EErvan Apsara BismakaNo ratings yet
- CBD Sirosis, Hematemesis MelenaDocument29 pagesCBD Sirosis, Hematemesis Melenadyah farahNo ratings yet
- 10.1007@s00405 020 06193 3Document6 pages10.1007@s00405 020 06193 3Anne SerneoNo ratings yet
- Comisión LancetDocument66 pagesComisión LancetKaya CromoNo ratings yet
- Leptospirosis CaseDocument29 pagesLeptospirosis CaseJp RectraNo ratings yet
- Eltroxin (New) TabDocument8 pagesEltroxin (New) TabhpradeepNo ratings yet
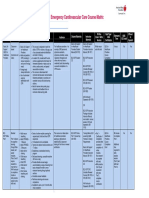
- Emergency Cardiovascular Care Course MatrixDocument15 pagesEmergency Cardiovascular Care Course MatrixJesus M. Espinosa EchavarriaNo ratings yet
- Handi Knee TapingDocument3 pagesHandi Knee TapingFadli NugrahaNo ratings yet
- Companies Dont Test in AnimalsDocument26 pagesCompanies Dont Test in AnimalsJoao BernardoNo ratings yet
- Implant OlogyDocument76 pagesImplant OlogyTaher RupawalaNo ratings yet
- Water Quality at Residential and Industrial AreaDocument11 pagesWater Quality at Residential and Industrial AreaMohamad AizanNo ratings yet
- Running Head: Client Teaching Wound Care 1Document3 pagesRunning Head: Client Teaching Wound Care 1Jerome Lazaro LumanogNo ratings yet
- Epilepsy 2015 A Practical Guide PDFDocument283 pagesEpilepsy 2015 A Practical Guide PDFrahma100% (1)
- The Attitudes and Beliefs About Over-the-Counter MedicinesDocument4 pagesThe Attitudes and Beliefs About Over-the-Counter MedicinesMahendra AvinashNo ratings yet