You might also like
- Innate ImmunityDocument9 pagesInnate Immunitynascha dumpNo ratings yet
- Lecture 2 Endocrine SystemDocument53 pagesLecture 2 Endocrine SystemLouella ArtatesNo ratings yet
- CH - 6, Vesicular TransportDocument29 pagesCH - 6, Vesicular TransportTony StarkNo ratings yet
- Physiology of Digestive SystemDocument70 pagesPhysiology of Digestive SystemVincent SerNo ratings yet
- Proteins MetabolismDocument27 pagesProteins MetabolismFouzia GillNo ratings yet
- GlycogenolysisDocument37 pagesGlycogenolysisJasmine Rey QuintoNo ratings yet
- Fisiologi 1 - Introducton Renal PhysiolgyDocument5 pagesFisiologi 1 - Introducton Renal PhysiolgyHachi Nini Shop IINo ratings yet
- Leucocytes 160619161725Document44 pagesLeucocytes 160619161725Rohit K Y100% (1)
- Lab Report Assistant Endocrine SystemDocument7 pagesLab Report Assistant Endocrine SystemJohn Louis AguilaNo ratings yet
- Aahar (Food) - Ayurvedic ConceptDocument27 pagesAahar (Food) - Ayurvedic ConceptRajendra Deshpande0% (1)
- The Fate of Metabolism Andmabolic PathwaysDocument25 pagesThe Fate of Metabolism Andmabolic PathwaysXuân Vi100% (1)
- Regulation of Blood GlucoseDocument21 pagesRegulation of Blood GlucoseDimple PatelNo ratings yet
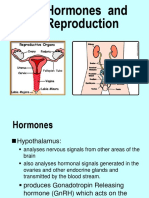
- (K9) Hormones and Reproduction 2 NanaDocument24 pages(K9) Hormones and Reproduction 2 NanaJane Andrea Christiano DjianzonieNo ratings yet
- Biochemistry Lecture 2 Cell and OrganellesDocument16 pagesBiochemistry Lecture 2 Cell and OrganellesProfessor Rakesh Sharma Biochemistry LecturesNo ratings yet
- L - 2 Physiology of Respiration IIDocument25 pagesL - 2 Physiology of Respiration IIkaukab azimNo ratings yet
- K-45 Pharmacology of Uterotonics & TocolyticsDocument55 pagesK-45 Pharmacology of Uterotonics & TocolyticsJane Andrea Christiano Djianzonie100% (1)
- Utmc - Utoledo.edu Depts Nursing Pdfs Basic EKG RefresherDocument210 pagesUtmc - Utoledo.edu Depts Nursing Pdfs Basic EKG RefresherTrish HồNo ratings yet
- (K4) Male Reproductive SystemDocument73 pages(K4) Male Reproductive SystemJane Andrea Christiano DjianzonieNo ratings yet
- Anatomy and Physiology: Prepared By: Ms. Irish SequihodDocument30 pagesAnatomy and Physiology: Prepared By: Ms. Irish SequihodMarie Fhel G OpenaNo ratings yet
- Gastrointestinal HormonesDocument46 pagesGastrointestinal HormonesTaufiq Singgih BaskoroNo ratings yet
- Lecture - 3 Properties of Cardiac MuscleDocument35 pagesLecture - 3 Properties of Cardiac MuscleMRM7MDNo ratings yet
- Amino Acid MetabolismDocument25 pagesAmino Acid MetabolismParixit BhandurgeNo ratings yet
- DNA Manipulative EnzymesDocument17 pagesDNA Manipulative EnzymesZain Ul AbedienNo ratings yet
- Heat Shock ProteinsDocument98 pagesHeat Shock ProteinsAprianie Wiwin100% (1)
- 1 RicketsDocument32 pages1 RicketsDarina Ismakaieva100% (1)
- Nervous System: Chapter # 7Document69 pagesNervous System: Chapter # 7saddam ud dinNo ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Anti Malarial DrugsDocument107 pagesAnti Malarial DrugsSindile MchunuNo ratings yet
- Experiment 4 (Biology)Document11 pagesExperiment 4 (Biology)言爱邦0% (1)
- ASIM M9Homeo Homeostasis 5E TEACHER NOTES, Revised 10/2015Document6 pagesASIM M9Homeo Homeostasis 5E TEACHER NOTES, Revised 10/2015Joshua WoodsNo ratings yet
- Answers To Questions: Activity 1: Assessing Starch Digestion by Salivary AmylaseDocument5 pagesAnswers To Questions: Activity 1: Assessing Starch Digestion by Salivary AmylaseTin-tinNo ratings yet
- Anatomy and Physiology of Digestive SystemDocument34 pagesAnatomy and Physiology of Digestive SystemIan IsidroNo ratings yet
- Chapter 8 - The VitaminsDocument3 pagesChapter 8 - The VitaminsYcell Latido100% (1)
- Endocrine System NotesDocument8 pagesEndocrine System NotesShiela Mae SagayoNo ratings yet
- Histo - Pituitary GlandDocument22 pagesHisto - Pituitary GlandRessam NazirNo ratings yet
- Differential White Blood Cell CountDocument20 pagesDifferential White Blood Cell CountNada hasan100% (2)
- The Muscular SystemDocument49 pagesThe Muscular SystemTessa Lonka TenidoNo ratings yet
- Endocrine System PhysiologyDocument2 pagesEndocrine System PhysiologyLuisGabitoNo ratings yet
- Neonatal SeizuresDocument22 pagesNeonatal SeizuresKatrin Marcelina SihombingNo ratings yet
- Pentose Phosphate PathwayDocument7 pagesPentose Phosphate PathwayElla BangalanNo ratings yet
- Dr. Khairun Nisa, Mkes., AIFO Fakultas Kedokteran Universitas Lampung 2014Document35 pagesDr. Khairun Nisa, Mkes., AIFO Fakultas Kedokteran Universitas Lampung 2014Riska WulandariNo ratings yet
- Urine Formation: Reabsorption and Secretion, and Water ConservationDocument5 pagesUrine Formation: Reabsorption and Secretion, and Water ConservationAshraf Moby100% (1)
- GIT NotesDocument23 pagesGIT NotesGrey SyNo ratings yet
- Physiology L6Document6 pagesPhysiology L6Anonymous elq7jZiSNo ratings yet
- Blood: Beenish Gul Khattak Lecturer Pharmacy Abasyn University PeshawarDocument66 pagesBlood: Beenish Gul Khattak Lecturer Pharmacy Abasyn University PeshawarEsperanza KtkNo ratings yet
- Female External GenitaliaDocument9 pagesFemale External Genitaliabuhari rabiuNo ratings yet
- The Human Body A Nutrition PerspectiveDocument50 pagesThe Human Body A Nutrition PerspectiveRichard GelmanNo ratings yet
- Theory Interacting N Open System ModelDocument23 pagesTheory Interacting N Open System ModelBheru LalNo ratings yet
- Enzymes (1ST Shifting) PDFDocument53 pagesEnzymes (1ST Shifting) PDFKwien AustriaNo ratings yet
- Clinical EnzymologyDocument25 pagesClinical Enzymologyaminata6No ratings yet
- Chapter25 Urinary SystemDocument9 pagesChapter25 Urinary Systemkikajet23No ratings yet
- Cell Biology and Genetics Notes On All Lectures PDFDocument62 pagesCell Biology and Genetics Notes On All Lectures PDFMR ManalangNo ratings yet
- Endo 3 Notes PDFDocument9 pagesEndo 3 Notes PDFDilNo ratings yet
- 1 IntroDocument5 pages1 IntroJeanjayannseptoemanNo ratings yet
- Anatomy of The Reproductive System EDocument4 pagesAnatomy of The Reproductive System EshreeNo ratings yet
- Presented By: DR Sharmila G SDocument76 pagesPresented By: DR Sharmila G SSharmila Shivakumar G SNo ratings yet
- Pancreatic Juice SecretionDocument3 pagesPancreatic Juice SecretionBilal SaidNo ratings yet
- Anatomy of Urinary SystemDocument34 pagesAnatomy of Urinary Systemhana100% (1)
- Lipids: Prepared By: de Torres, Angelica M. Che-4102Document37 pagesLipids: Prepared By: de Torres, Angelica M. Che-4102Angelica de TorresNo ratings yet
- SGD Physiology Endocrine and MetabolismDocument7 pagesSGD Physiology Endocrine and MetabolismTinesh RajahNo ratings yet
- Digestive System NotesDocument10 pagesDigestive System NotesArchanna VyassNo ratings yet
- Reproductive PhysiologyDocument40 pagesReproductive PhysiologyBaiq Trisna Satriana100% (1)
- Principles of Anatomy and Physiology: 14 EditionDocument62 pagesPrinciples of Anatomy and Physiology: 14 EditionWilliam C Chisha100% (1)
- Lecture 1 - Introduction To HematologyDocument30 pagesLecture 1 - Introduction To Hematologyimam100% (1)
- Rest and SleepDocument11 pagesRest and Sleepdlneisha61No ratings yet
- Thyroid and Parathyroid GlandsDocument23 pagesThyroid and Parathyroid Glandsmoimoi819No ratings yet
- Basic EKG RefresherDocument57 pagesBasic EKG RefresherJane Andrea Christiano DjianzonieNo ratings yet
- En GoutDocument2 pagesEn GoutJane Andrea Christiano DjianzonieNo ratings yet
- SIMAK Pascasarjana S1 Ekstensi 2012 ENGLISH Kode 201Document20 pagesSIMAK Pascasarjana S1 Ekstensi 2012 ENGLISH Kode 201pLangpLingpLungNo ratings yet
- En GoutDocument2 pagesEn GoutJane Andrea Christiano DjianzonieNo ratings yet
- Bab 150 Hemopoesis PDFDocument3 pagesBab 150 Hemopoesis PDFJane Andrea Christiano DjianzonieNo ratings yet
- K - 65 Farmakodinamik Dan Farmakokinetik Kontrasepsi TDocument24 pagesK - 65 Farmakodinamik Dan Farmakokinetik Kontrasepsi TJane Andrea Christiano DjianzonieNo ratings yet
- K.7 & 8 Hormone Reproductive SystDocument55 pagesK.7 & 8 Hormone Reproductive SystsutansikandarNo ratings yet
- (K11-K12) Fisiologi KehamilanDocument76 pages(K11-K12) Fisiologi KehamilanJane Andrea Christiano DjianzonieNo ratings yet
- Blok Reproductive System: Prof. Dr. Abdul Rasyid, Sprad, PHDDocument46 pagesBlok Reproductive System: Prof. Dr. Abdul Rasyid, Sprad, PHDJane Andrea Christiano DjianzonieNo ratings yet
- Blok Reproductive System: Prof. Dr. Abdul Rasyid, Sprad, PHDDocument46 pagesBlok Reproductive System: Prof. Dr. Abdul Rasyid, Sprad, PHDJane Andrea Christiano DjianzonieNo ratings yet
- K 74-75 Pathology of UterusDocument51 pagesK 74-75 Pathology of UterusJane Andrea Christiano Djianzonie100% (1)
- (k10) Ginecologic ExaminationDocument23 pages(k10) Ginecologic ExaminationJane Andrea Christiano DjianzonieNo ratings yet
- K 7 - 9 Hormone Reproductive Syst.Document52 pagesK 7 - 9 Hormone Reproductive Syst.Jane Andrea Christiano DjianzonieNo ratings yet
- (k10) Ginecologic ExaminationDocument23 pages(k10) Ginecologic ExaminationJane Andrea Christiano DjianzonieNo ratings yet
- (K5-K6) Hormon Repro Pria Dan Wanita, EditDocument53 pages(K5-K6) Hormon Repro Pria Dan Wanita, EditJane Andrea Christiano DjianzonieNo ratings yet
- Ovarian Carsinoma (KBK)Document25 pagesOvarian Carsinoma (KBK)Jane Andrea Christiano DjianzonieNo ratings yet
- (K2) Histo Female Reproductive System 2012Document81 pages(K2) Histo Female Reproductive System 2012Jane Andrea Christiano DjianzonieNo ratings yet
- K 5-6 Fungsi Hormone ReproduksiDocument54 pagesK 5-6 Fungsi Hormone ReproduksiJane Andrea Christiano DjianzonieNo ratings yet
- Physiology of Pregnancy: Department of Physiology School of Medicine University of Sumatera UtaraDocument80 pagesPhysiology of Pregnancy: Department of Physiology School of Medicine University of Sumatera UtaraJane Andrea Christiano DjianzonieNo ratings yet
- Vulvar Casinoma (KBK)Document22 pagesVulvar Casinoma (KBK)Jane Andrea Christiano Djianzonie100% (1)
- K - 12 Candidiasis (Mikrobiologi)Document38 pagesK - 12 Candidiasis (Mikrobiologi)Vedora Angelia GultomNo ratings yet
- k8 Biokim Hormon GdsDocument35 pagesk8 Biokim Hormon GdsRobert HallNo ratings yet
- Neonatology Division Department of Child Health Medical School University of Sumatera UtaraDocument22 pagesNeonatology Division Department of Child Health Medical School University of Sumatera UtaraJane Andrea Christiano DjianzonieNo ratings yet
- Gestational Trophoblastic Neoplasia (KBK)Document22 pagesGestational Trophoblastic Neoplasia (KBK)Jane Andrea Christiano DjianzonieNo ratings yet
- GDS K-6 - Newborn Physical ExaminationDocument44 pagesGDS K-6 - Newborn Physical ExaminationJosephine IrenaNo ratings yet
- K.3b HORMONE CONTROL OF GROWTHDocument22 pagesK.3b HORMONE CONTROL OF GROWTHJane Andrea Christiano DjianzonieNo ratings yet
- ks3 8a Eq Nutrition and Digestion 69marks 15pgs TbaseDocument15 pagesks3 8a Eq Nutrition and Digestion 69marks 15pgs TbaseAbby ChauNo ratings yet
- Alimentary SystemDocument51 pagesAlimentary SystemKavivarma Raj RajendranNo ratings yet
- Sa I Class X Science 3Document21 pagesSa I Class X Science 3cpverma2811No ratings yet
- Ann 202 212 Vle Funaab 2Document80 pagesAnn 202 212 Vle Funaab 2KAWE-EDU CONSULTSNo ratings yet
- EnzymesDocument13 pagesEnzymesManjusha KondepudiNo ratings yet
- Digestion & Absorption ProteinsDocument44 pagesDigestion & Absorption ProteinsPutri Indah NirmalasariNo ratings yet
- Pepsin As A Case Study For Method and Unit Harmonization: Industry PerspectiveDocument27 pagesPepsin As A Case Study For Method and Unit Harmonization: Industry PerspectiveUtik PurwantiNo ratings yet
- Aipmt-2008 Screening-With SolutionsDocument57 pagesAipmt-2008 Screening-With Solutionsapi-19826463100% (1)
- 2019-AGA-DDSEP-9-Chapter-2-1557871764749 1 ENFERMEDADES DEL ESTOMAGODocument24 pages2019-AGA-DDSEP-9-Chapter-2-1557871764749 1 ENFERMEDADES DEL ESTOMAGOEmilia GarciaNo ratings yet
- Ebf 303 Environmental and Animal PhysiologyDocument61 pagesEbf 303 Environmental and Animal PhysiologyAngela BrownNo ratings yet
- Pplied Enzymology: Enzyme SourcesDocument51 pagesPplied Enzymology: Enzyme SourcesMaha hameedNo ratings yet
- SIM Biochemistry ULO7Document12 pagesSIM Biochemistry ULO7Darl MalazarteNo ratings yet
- PEX 08 03 Dikonversi DikonversiDocument4 pagesPEX 08 03 Dikonversi Dikonversishinji longreyNo ratings yet
- Antacids Class 12Document7 pagesAntacids Class 12rav_rkdNo ratings yet
- Monitoring The Activity of Feed Enzymes in Vitro PDFDocument6 pagesMonitoring The Activity of Feed Enzymes in Vitro PDFВалерий КрюковNo ratings yet
- IBMSDocument73 pagesIBMSRugene Naragas BeratoNo ratings yet
- Lab12 Fisiología DigestivaDocument7 pagesLab12 Fisiología DigestivacesamavNo ratings yet
- HCL Secretion in StomachDocument5 pagesHCL Secretion in StomachKhalid HasanNo ratings yet
- Cambridge IGCSE ™: Biology 0610/42 October/November 2022Document15 pagesCambridge IGCSE ™: Biology 0610/42 October/November 2022dharshini_perumalNo ratings yet
- Digestion and Absorption: Fact/Definition Type QuestionsDocument9 pagesDigestion and Absorption: Fact/Definition Type QuestionsNayan BhardwazNo ratings yet
- Life Process Nutrition Question 1Document3 pagesLife Process Nutrition Question 1Nakshatra PaliwalNo ratings yet
- Enzyme Catalysis LabDocument8 pagesEnzyme Catalysis LabAzra RamicNo ratings yet
- Week 14: Digestion Chemistry: Intrinsic FactorDocument4 pagesWeek 14: Digestion Chemistry: Intrinsic FactorLore Anne Mhae SantosNo ratings yet
- 1-Human Physiology Digestion Absorption PDFDocument29 pages1-Human Physiology Digestion Absorption PDFPintu KarmakarNo ratings yet
- Acute Gastritis CiciDocument43 pagesAcute Gastritis CiciDwi Rezky AmaliaNo ratings yet
- Simulating Human DigestionDocument35 pagesSimulating Human DigestionLIBARDO CASTAÑEDA FLOREZNo ratings yet