You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Building2014 MarchDocument146 pagesBuilding2014 Marcharnav saikiaNo ratings yet
- Bathtubs PDFDocument26 pagesBathtubs PDFJasleenKaurNo ratings yet
- Institute of MountaineeringDocument22 pagesInstitute of MountaineeringJasleenKaurNo ratings yet
- Building Forms and Features On Hilly AreDocument25 pagesBuilding Forms and Features On Hilly ArepurvabhagtNo ratings yet
- ChronicBabe HowareyouDocument8 pagesChronicBabe HowareyouPerfect_Two100% (1)
- Mountaineering Training Institute at Dal PDFDocument41 pagesMountaineering Training Institute at Dal PDFJasleenKaur100% (1)
- Foundations Ch4Document62 pagesFoundations Ch4stevehuppertNo ratings yet
- 4 Season Hotel and ResortDocument11 pages4 Season Hotel and ResortJasleenKaurNo ratings yet
- Detailed Project Report for Slum Redevelopment of Bagrana SlumDocument62 pagesDetailed Project Report for Slum Redevelopment of Bagrana SlumJasleenKaur0% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chap1 HRM581 Oct Feb 2023Document20 pagesChap1 HRM581 Oct Feb 2023liana bahaNo ratings yet
- Tona Totka To Achieve Self Objectives - Happy and Prosperous Married Life and Smooth Marriage, Get Married Without Any ProblemsDocument8 pagesTona Totka To Achieve Self Objectives - Happy and Prosperous Married Life and Smooth Marriage, Get Married Without Any Problemsvinitkgupta0% (1)
- Vodafone service grievance unresolvedDocument2 pagesVodafone service grievance unresolvedSojan PaulNo ratings yet
- WADVDocument2 pagesWADVANNA MARY GINTORONo ratings yet
- CHEM205 Review 8Document5 pagesCHEM205 Review 8Starlyn RodriguezNo ratings yet
- Asset To LiabDocument25 pagesAsset To LiabHavanaNo ratings yet
- (Cooperative) BOD and Secretary CertificateDocument3 pages(Cooperative) BOD and Secretary Certificateresh lee100% (1)
- Religious Marriage in A Liberal State Gidi Sapir & Daniel StatmanDocument26 pagesReligious Marriage in A Liberal State Gidi Sapir & Daniel StatmanR Hayim BakaNo ratings yet
- Court rules on nullification of title in ejectment caseDocument1 pageCourt rules on nullification of title in ejectment caseNapolyn FernandezNo ratings yet
- Software Project Sign-Off DocumentDocument7 pagesSoftware Project Sign-Off DocumentVocika MusixNo ratings yet
- JNMF Scholarship Application Form-1Document7 pagesJNMF Scholarship Application Form-1arudhayNo ratings yet
- High-Performance Work Practices: Labor UnionDocument2 pagesHigh-Performance Work Practices: Labor UnionGabriella LomanorekNo ratings yet
- Project Report Final PDFDocument74 pagesProject Report Final PDFSaurav KumarNo ratings yet
- MUN Resolution For The North Korean Missile CrisisDocument2 pagesMUN Resolution For The North Korean Missile CrisissujalachamNo ratings yet
- Vivarium - Vol 37, Nos. 1-2, 1999Document306 pagesVivarium - Vol 37, Nos. 1-2, 1999Manticora VenerabilisNo ratings yet
- Aristotle Model of CommunicationDocument4 pagesAristotle Model of CommunicationSem BulagaNo ratings yet
- Syllabus For M. Phil. Course Part - I Paper - I Title: General Survey of Buddhism in India and Abroad 100 Marks Section - ADocument6 pagesSyllabus For M. Phil. Course Part - I Paper - I Title: General Survey of Buddhism in India and Abroad 100 Marks Section - ASunil SNo ratings yet
- Valuing Human Capital at Infosys Using Lev & Schwartz ModelDocument3 pagesValuing Human Capital at Infosys Using Lev & Schwartz ModelAnchal Jain100% (2)
- 5 8 Pe Ola) CSL, E Quranic WondersDocument280 pages5 8 Pe Ola) CSL, E Quranic WondersMuhammad Faizan Raza Attari QadriNo ratings yet
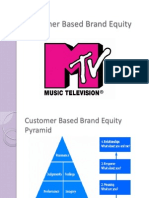
- Customer Based Brand EquityDocument13 pagesCustomer Based Brand EquityZeeshan BakshiNo ratings yet
- A Bibliography of China-Africa RelationsDocument233 pagesA Bibliography of China-Africa RelationsDavid Shinn100% (1)
- CEI KAH OCT v1Document1 pageCEI KAH OCT v1Francis Ho HoNo ratings yet
- In Bengal, Erosion Leads To Land Loss: Shiv Sahay SinghDocument1 pageIn Bengal, Erosion Leads To Land Loss: Shiv Sahay SinghRohith KumarNo ratings yet
- AIESEC Experience-MBC 2016Document25 pagesAIESEC Experience-MBC 2016Karina AnantaNo ratings yet
- Mx. Gad 2023Document3 pagesMx. Gad 2023Wany BerryNo ratings yet
- Sabbia Food MenuDocument2 pagesSabbia Food MenuNell CaseyNo ratings yet
- VI Sem. BBA - HRM Specialisation - Human Resource Planning and Development PDFDocument39 pagesVI Sem. BBA - HRM Specialisation - Human Resource Planning and Development PDFlintameyla50% (2)
- Effecting Organizational Change PresentationDocument23 pagesEffecting Organizational Change PresentationSvitlanaNo ratings yet
- B SDocument36 pagesB SkeithguruNo ratings yet
- Winny Chepwogen CVDocument16 pagesWinny Chepwogen CVjeff liwaliNo ratings yet