You might also like
- Chest Physiotherapy or Techniques in Cardio Pulmonary Physiotherapy A Running CommentaryDocument5 pagesChest Physiotherapy or Techniques in Cardio Pulmonary Physiotherapy A Running CommentaryGopi KrishnanNo ratings yet
- 1Document4 pages1Gopi KrishnanNo ratings yet
- Informed ConsentDocument1 pageInformed ConsentGopi KrishnanNo ratings yet
- Background and ObjectivesDocument2 pagesBackground and ObjectivesGopi KrishnanNo ratings yet
- UgqsuguwsgugixhiDocument1 pageUgqsuguwsgugixhiGopi KrishnanNo ratings yet
- Gopikrishnan.C.G: Career ObjectiveDocument4 pagesGopikrishnan.C.G: Career ObjectiveGopi KrishnanNo ratings yet
- ConferenceDocument1 pageConferenceGopi KrishnanNo ratings yet
- VishakDocument2 pagesVishakGopi KrishnanNo ratings yet
- UgqsuguwsgugixhiDocument1 pageUgqsuguwsgugixhiGopi KrishnanNo ratings yet
- FythqsgxchcsxjDocument1 pageFythqsgxchcsxjGopi KrishnanNo ratings yet
- Acknowledgement: and Sports Medicine), Vice Principal, Bethany Navajeevan College of Physiotherapy, For HerDocument1 pageAcknowledgement: and Sports Medicine), Vice Principal, Bethany Navajeevan College of Physiotherapy, For HerGopi KrishnanNo ratings yet
- MET knee extension testsDocument7 pagesMET knee extension testsGopi KrishnanNo ratings yet
- Informed ConsentDocument1 pageInformed ConsentGopi KrishnanNo ratings yet
- LefsDocument1 pageLefsGopi KrishnanNo ratings yet
- Gopi KrishnanDocument1 pageGopi KrishnanGopi KrishnanNo ratings yet
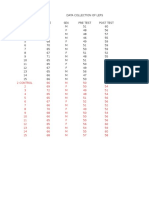
- Name: Age: Sex: Date:: Data Collection SheetDocument1 pageName: Age: Sex: Date:: Data Collection SheetGopi KrishnanNo ratings yet
- Comparative Study Between Muscle Energy Techinque and Eccentric Training in Improving Hamstring Muscle Flexibility and Performance in Male College Athlete1Document3 pagesComparative Study Between Muscle Energy Techinque and Eccentric Training in Improving Hamstring Muscle Flexibility and Performance in Male College Athlete1Gopi KrishnanNo ratings yet
- GOPIKRISHNANDocument1 pageGOPIKRISHNANGopi KrishnanNo ratings yet
- Physiotherapy in Orthopeadic ConditionsDocument2 pagesPhysiotherapy in Orthopeadic ConditionsGopi KrishnanNo ratings yet
- Brochure PDFDocument2 pagesBrochure PDFGopi KrishnanNo ratings yet
- Ygwq 89 Yp UP8 ADocument1 pageYgwq 89 Yp UP8 AGopi KrishnanNo ratings yet
- 719 SMA InjuryBrochure Hamstring - Web PDFDocument4 pages719 SMA InjuryBrochure Hamstring - Web PDFGopi KrishnanNo ratings yet
- Critical care approach to poisoned patientsDocument90 pagesCritical care approach to poisoned patientsGopi KrishnanNo ratings yet
- The Use of Surface Electromyography in Biomechanics PDFDocument29 pagesThe Use of Surface Electromyography in Biomechanics PDFRaul Enrique Castillo VeraNo ratings yet
- ARDS GuidelinesDocument18 pagesARDS GuidelinesGopi KrishnanNo ratings yet
- Posterior Cruciate Ligament InjuriesDocument26 pagesPosterior Cruciate Ligament InjuriesGopi KrishnanNo ratings yet
- 212700554/sport Speed and Agility Training 2dnDocument1 page212700554/sport Speed and Agility Training 2dnGopi KrishnanNo ratings yet
- Critical care approach to poisoned patientsDocument90 pagesCritical care approach to poisoned patientsGopi KrishnanNo ratings yet
- Cardiac SupportDocument8 pagesCardiac SupportGopi KrishnanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hagiwara, 2017Document13 pagesHagiwara, 2017luccafcms56No ratings yet
- Cardiac RehabilitationDocument48 pagesCardiac RehabilitationsdsdNo ratings yet
- College of Nursing: (Dalubhasaan NG Narsing)Document4 pagesCollege of Nursing: (Dalubhasaan NG Narsing)Anna Sofia ReyesNo ratings yet
- What Is Cardiogenic Shock?Document3 pagesWhat Is Cardiogenic Shock?nipheyy dananNo ratings yet
- Cardiac CatheterizationDocument6 pagesCardiac Catheterizationgurneet kourNo ratings yet
- Sample ReportDocument3 pagesSample ReportRobeants Charles PierreNo ratings yet
- Association of Variability in Uric Acid and Future CliDocument7 pagesAssociation of Variability in Uric Acid and Future Clinguyenthanhluan2801No ratings yet
- PericardiocentesisDocument3 pagesPericardiocentesisThe Multilingual MedicNo ratings yet
- Cardiology The ABC's of The PQRSTDocument2 pagesCardiology The ABC's of The PQRSTMardiya MahmoudNo ratings yet
- How To Analyze EkgsDocument40 pagesHow To Analyze EkgsJosh WeisNo ratings yet
- Double-Outlet Left Ventricle and Vascular MalformationsDocument3 pagesDouble-Outlet Left Ventricle and Vascular MalformationsRaul UrietaNo ratings yet
- 4 - CASA - 2017 The Cardiac Arrest Sonofraphic AssessmemtDocument4 pages4 - CASA - 2017 The Cardiac Arrest Sonofraphic AssessmemtFernando YaksicNo ratings yet
- Hemodynamic MonitoringDocument10 pagesHemodynamic MonitoringDivya Joy100% (1)
- What Is A Normal Pulse Rate - Heart Matters Magazine BHFDocument1 pageWhat Is A Normal Pulse Rate - Heart Matters Magazine BHFabdullahNo ratings yet
- Mi 2Document8 pagesMi 2Aiman ArifinNo ratings yet
- Acls FixDocument20 pagesAcls Fixluthfi adityaNo ratings yet
- Document 30Document7 pagesDocument 30SNIGDHA PATLOLANo ratings yet
- Module 1 Case StudyDocument5 pagesModule 1 Case Studyapi-564432337100% (1)
- (The European Society of Cardiology Series) Jose Luis Zamorano, Jeroen Bax, Juhani Knuuti, Patrizio Lancellotti, Fausto Pinto, Bogdan A. Popescu, Udo Sechtem - The ESC Textbook of Cardiovascular ImagiDocument865 pages(The European Society of Cardiology Series) Jose Luis Zamorano, Jeroen Bax, Juhani Knuuti, Patrizio Lancellotti, Fausto Pinto, Bogdan A. Popescu, Udo Sechtem - The ESC Textbook of Cardiovascular ImagiEdu MartinsNo ratings yet
- Yashwanth - IHD HFrEfDocument16 pagesYashwanth - IHD HFrEfYashwanth N BNo ratings yet
- The Electrocardiogram: Ecg: by Gaurishi Agarwal, 32Document17 pagesThe Electrocardiogram: Ecg: by Gaurishi Agarwal, 32Gaurishi AgarwalNo ratings yet
- CVS ExamDocument35 pagesCVS Examtravis efraimNo ratings yet
- The CardiacDocument7 pagesThe CardiacCake ManNo ratings yet
- Insuficiencia Cardiaca Neyssa KimeeDocument33 pagesInsuficiencia Cardiaca Neyssa KimeeNEYSSA KIMEE SAINT VILNo ratings yet
- Echocardiography & Color Doppler Report Measurements Absolute Value Normals Absolute / MDocument3 pagesEchocardiography & Color Doppler Report Measurements Absolute Value Normals Absolute / MAmol PandeyNo ratings yet
- ST Segment ElevationsDocument114 pagesST Segment ElevationsMuruganandham RNo ratings yet
- Types of StrokeDocument12 pagesTypes of Strokefakher adnanNo ratings yet
- Diagnostic Evaluation of The HeartDocument3 pagesDiagnostic Evaluation of The HeartClaire GidoNo ratings yet
- Radiol 223008Document15 pagesRadiol 223008rehan hayderNo ratings yet
- QUIZ Acute-Myocardial-InfarctionDocument3 pagesQUIZ Acute-Myocardial-InfarctionErika Joille PatayonNo ratings yet