You might also like
- Critical Care Drugs OverviewDocument23 pagesCritical Care Drugs OverviewAsri Ernadi100% (1)
- Mitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandMitral Valve Regurgitation, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Advanced Airway Care: Intensive Care Unit PerspectiveDocument42 pagesAdvanced Airway Care: Intensive Care Unit PerspectiveJeffery Samuel100% (1)
- Vasoactive DrugsDocument61 pagesVasoactive DrugsAde Gustina SiahaanNo ratings yet
- HW InotropesDocument3 pagesHW InotropesNatalie YeohNo ratings yet
- ACLS Algorithms Adult 2010 Revised May 31 2011Document12 pagesACLS Algorithms Adult 2010 Revised May 31 2011arturschander3614No ratings yet
- Prehospital MedicationsDocument123 pagesPrehospital Medicationshilwaalfi100% (1)
- ACC/AHA STEMI GuidelinesDocument94 pagesACC/AHA STEMI GuidelinesDika DekokNo ratings yet
- Acls Course HandoutsDocument8 pagesAcls Course HandoutsRoxas CedrickNo ratings yet
- Cardiac MedicationsDocument8 pagesCardiac Medicationsangeline totaram100% (2)
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet
- Adult Infusion StandardsDocument11 pagesAdult Infusion StandardsJessica Torreglosa100% (1)
- 02 AntiarrhythmicAgentsDocument83 pages02 AntiarrhythmicAgentsSiddhant BanwatNo ratings yet
- Normal DIE CPP Calculations:: Increased Intracranial Pressure (Cerebral Perfusion Pressure)Document79 pagesNormal DIE CPP Calculations:: Increased Intracranial Pressure (Cerebral Perfusion Pressure)Nur SanaaniNo ratings yet
- Arrhythmia 2Document31 pagesArrhythmia 2rittvedNo ratings yet
- ED Dilution Guide 2018 - Jan 2019Document42 pagesED Dilution Guide 2018 - Jan 2019asyrafrusydi9901No ratings yet
- Paramedic Exam Guide to Immunizations & Research MethodsDocument21 pagesParamedic Exam Guide to Immunizations & Research MethodsBarry GruenbaumNo ratings yet
- Management of Shock: Role of Inotropic & Vasoactive DrugsDocument50 pagesManagement of Shock: Role of Inotropic & Vasoactive DrugsbajaocNo ratings yet
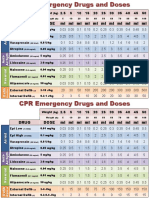
- CPR Emergency Drug DosesDocument2 pagesCPR Emergency Drug DosesCote ParejaNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Anxiolytic and Hypnotic AgentsDocument50 pagesAnxiolytic and Hypnotic AgentsMoxie Macado100% (1)
- VASOACTIVE THERAPY GUIDE FOR CRITICALLY ILL PATIENTSDocument26 pagesVASOACTIVE THERAPY GUIDE FOR CRITICALLY ILL PATIENTSlidya agustin100% (1)
- ACLS Secondary Survey For A Patient in Respiratory Arrest: BLS Arrest Figure 1. Basic Life Support Primary SurveyDocument30 pagesACLS Secondary Survey For A Patient in Respiratory Arrest: BLS Arrest Figure 1. Basic Life Support Primary SurveyLusia NataliaNo ratings yet
- DX Alcohol Withdrawal PDFDocument3 pagesDX Alcohol Withdrawal PDFSherree Hayes100% (1)
- AirCare Pediatric Reference GuideDocument8 pagesAirCare Pediatric Reference GuideN/ANo ratings yet
- Marvel Regional Health Network Risk Assessment Power PointDocument18 pagesMarvel Regional Health Network Risk Assessment Power Pointapi-682342806No ratings yet
- Medications Used in Code Blue EmergenciesDocument24 pagesMedications Used in Code Blue EmergenciesAhmed Ali Mohammed AlbashirNo ratings yet
- Assessment Algorithm For Sedated Adult ICU Patients: No YesDocument18 pagesAssessment Algorithm For Sedated Adult ICU Patients: No YeshendraNo ratings yet
- Inotropes, Excellent Article, With DosingDocument47 pagesInotropes, Excellent Article, With DosingNavojit ChowdhuryNo ratings yet
- Guide to Respiratory Exam - OSCE ChecklistDocument33 pagesGuide to Respiratory Exam - OSCE ChecklistBasmah 7No ratings yet
- Drugs Commonly Available in The Critical Care UnitDocument10 pagesDrugs Commonly Available in The Critical Care UnitEggy PascualNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Module # 5 Pharmacology NursingDocument45 pagesModule # 5 Pharmacology Nursingannyeong_123No ratings yet
- Internship Manual For MBBSDocument29 pagesInternship Manual For MBBSKoustav ChakrabortyNo ratings yet
- HFandVADRoleDocument34 pagesHFandVADRoleJohnNo ratings yet
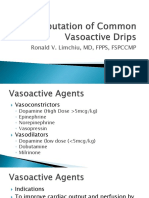
- Computation of Common Vasoactive DripsDocument23 pagesComputation of Common Vasoactive DripsRoxanneGailBigcasGoleroNo ratings yet
- ACLS Primary Survey Guide for Respiratory ArrestDocument34 pagesACLS Primary Survey Guide for Respiratory Arrest강기연100% (1)
- MN105613 PICU2022 Book ProofDocument60 pagesMN105613 PICU2022 Book ProofErwin Dela GanaNo ratings yet
- ECMO and Right Ventricular FailureDocument9 pagesECMO and Right Ventricular FailureLuis Fernando Morales JuradoNo ratings yet
- Arterial Blood GasesDocument9 pagesArterial Blood GasesJohn BattleNo ratings yet
- West Visayas State University: Nursing ProcessDocument4 pagesWest Visayas State University: Nursing ProcessPhylum Chordata100% (1)
- Anasthetic DrugsDocument62 pagesAnasthetic DrugsMilda InayahNo ratings yet
- Best Vasopressor For Advanced Vasodilatory Shock Should Vasopressin Be Part of The MixDocument4 pagesBest Vasopressor For Advanced Vasodilatory Shock Should Vasopressin Be Part of The MixSurachai PraimaiNo ratings yet
- Invasive Devices On CXRDocument1 pageInvasive Devices On CXRLaurensia Erlina NataliaNo ratings yet
- Management of Arterial LineDocument16 pagesManagement of Arterial LineFarcasanu Liana GeorgianaNo ratings yet
- Stroke: AHA/ASA Guidelines For The Early Management of Patients With Acute Ischemic Stroke (2019)Document14 pagesStroke: AHA/ASA Guidelines For The Early Management of Patients With Acute Ischemic Stroke (2019)Natalia OrtizNo ratings yet
- Journal ClubDocument26 pagesJournal Clubysindhura23gmailcom100% (1)
- Stroke Pathway For Acute Care ProvidersDocument5 pagesStroke Pathway For Acute Care Providersdremad1974100% (1)
- Capnography and Its ApplicationsDocument37 pagesCapnography and Its ApplicationsTraceNo ratings yet
- A Batch Time Table 1Document2 pagesA Batch Time Table 1Vijayan VelayudhanNo ratings yet
- Amritha I ST Year MBBS Result 2019Document7 pagesAmritha I ST Year MBBS Result 2019Vijayan VelayudhanNo ratings yet
- Thorax SpottersDocument10 pagesThorax SpottersVijayan Velayudhan100% (1)
- Q@Ffii: National CalicutDocument3 pagesQ@Ffii: National Calicutbhanuprakash KommineniNo ratings yet
- Spotters by DR Deepa Sivaraj..Document20 pagesSpotters by DR Deepa Sivaraj..Vijayan VelayudhanNo ratings yet
- Semester 1 Civil SylubusDocument8 pagesSemester 1 Civil SylubusVijayan VelayudhanNo ratings yet
- Anatomy Embryology MBBS 2017Document24 pagesAnatomy Embryology MBBS 2017Vijayan VelayudhanNo ratings yet
- Collection of University Question Paper 1990-2016 Mbbs - 2 YearDocument51 pagesCollection of University Question Paper 1990-2016 Mbbs - 2 YearVijayan Velayudhan100% (1)
- Thorax SpottersDocument10 pagesThorax SpottersVijayan VelayudhanNo ratings yet
- CamScanner Scans - Multiple PagesDocument13 pagesCamScanner Scans - Multiple PagesVijayan Velayudhan100% (3)
- First Year BTech CurriculumDocument20 pagesFirst Year BTech CurriculumNanditha ANo ratings yet
- Schedule - Orientation Programme - BTech Civil - 2020Document1 pageSchedule - Orientation Programme - BTech Civil - 2020Vijayan VelayudhanNo ratings yet
- Academic Calendar - Monsoon-2020-2021 - 2020 Admission UGDocument1 pageAcademic Calendar - Monsoon-2020-2021 - 2020 Admission UGBvs TejaNo ratings yet
- Syllabus BriefDocument41 pagesSyllabus BriefYedu RajNo ratings yet
- Syllabus BriefDocument41 pagesSyllabus BriefYedu RajNo ratings yet
- Academic Calendar - Monsoon-2020-2021 - 2020 Admission UGDocument1 pageAcademic Calendar - Monsoon-2020-2021 - 2020 Admission UGBvs TejaNo ratings yet
- First Year BTech CurriculumDocument20 pagesFirst Year BTech CurriculumNanditha ANo ratings yet
- How NCERT Books Can Help You Prepare For AIPMT 2016Document3 pagesHow NCERT Books Can Help You Prepare For AIPMT 2016Vijayan VelayudhanNo ratings yet
- CBSE 12 Class 12th Mark SchemeDocument2 pagesCBSE 12 Class 12th Mark SchemeVijayan VelayudhanNo ratings yet
- English Communicative: Summative Assessment - Ii, 2014Document8 pagesEnglish Communicative: Summative Assessment - Ii, 2014Vijayan VelayudhanNo ratings yet
- Class 11 Biology NotesDocument8 pagesClass 11 Biology NotesVijayan Velayudhan100% (2)
- Lesson PlanDocument11 pagesLesson PlanVijayan Velayudhan100% (1)
- Demodex CanisDocument19 pagesDemodex Canisapi-337841627No ratings yet
- HYDRONEPHROSISDocument43 pagesHYDRONEPHROSISEureka RathinamNo ratings yet
- Maternity Clinical Network Contact DetailsDocument18 pagesMaternity Clinical Network Contact DetailsAlina-Gabriela MarinNo ratings yet
- Pantoea Agglomerans - ADocument9 pagesPantoea Agglomerans - AmadelaineNo ratings yet
- Osteocaps 0.25mcgDocument1 pageOsteocaps 0.25mcginnolpacNo ratings yet
- Use of Local and Axial Pattern Flaps For Reconstruction of The Hard and Soft Palate PDFDocument9 pagesUse of Local and Axial Pattern Flaps For Reconstruction of The Hard and Soft Palate PDFJose Luis Granados SolerNo ratings yet
- Unconventional Fixed Partial Denture: A Simple Solution For Aesthetic RehabilitationDocument4 pagesUnconventional Fixed Partial Denture: A Simple Solution For Aesthetic RehabilitationAdvanced Research PublicationsNo ratings yet
- Blood Banking and Transfusion Medicine Practice QuestionsDocument45 pagesBlood Banking and Transfusion Medicine Practice QuestionsVincent Reyes85% (40)
- AHF Timeline InfographicDocument7 pagesAHF Timeline InfographicNovartisNewsroomNo ratings yet
- Intussusception Pedia ReportDocument13 pagesIntussusception Pedia ReportJesselyn HeruelaNo ratings yet
- Staph Lecture MicrococcusDocument30 pagesStaph Lecture Micrococcussophia salibaNo ratings yet
- Chorea Continuum 2019Document35 pagesChorea Continuum 2019nicolasNo ratings yet
- Treatment of Endometriosis in Women Desiring FertilityDocument23 pagesTreatment of Endometriosis in Women Desiring FertilityVaisnavi Muthoovaloo67% (3)
- Pharmacology Lab (1) : Routes of Drug AdministrationDocument14 pagesPharmacology Lab (1) : Routes of Drug AdministrationBotan AbdullahNo ratings yet
- Pharmacology and The Older AdultDocument26 pagesPharmacology and The Older AdultJether Joy Hyacinth VelardeNo ratings yet
- Respiratory Procedures: Tracheal Intubation PreparationDocument46 pagesRespiratory Procedures: Tracheal Intubation PreparationRhea Andrea UyNo ratings yet
- Arterial DiseaseDocument191 pagesArterial DiseaseAura DiscyacittaNo ratings yet
- A Prospective Study On Acute Limb Ischemia - Presentation, Management, Outcome - Our Institutional ExperienceDocument6 pagesA Prospective Study On Acute Limb Ischemia - Presentation, Management, Outcome - Our Institutional ExperienceIJAR JOURNALNo ratings yet
- Comparison of Bupivacaine-Dexmedetomidine VS Bupivacaine-Fentanyl VS Bupivacaine - Saline For Unilateral Spinal Anaesthesia in Lower Limb SurgeryDocument9 pagesComparison of Bupivacaine-Dexmedetomidine VS Bupivacaine-Fentanyl VS Bupivacaine - Saline For Unilateral Spinal Anaesthesia in Lower Limb SurgeryIJAR JOURNALNo ratings yet
- Welcome To The Era of Universal Airway Management: EditorialDocument5 pagesWelcome To The Era of Universal Airway Management: EditorialHugo Robles GómezNo ratings yet
- Comparative-Study-Of-Four-Methods-Of-Clinical-Estimation-Of-Fetal-Weight 2Document9 pagesComparative-Study-Of-Four-Methods-Of-Clinical-Estimation-Of-Fetal-Weight 2Abegail Fermanejo-GeneraoNo ratings yet
- Nephritic SyndromeDocument19 pagesNephritic SyndromesangheetaNo ratings yet
- TUBERCULOSISDocument16 pagesTUBERCULOSISfranciz CalagoNo ratings yet
- For The Best Sinus Congestion RemediesDocument4 pagesFor The Best Sinus Congestion Remedies4zaleakuNo ratings yet
- The Pelvic Floor and Core ExercisesDocument4 pagesThe Pelvic Floor and Core ExercisesJeffrey PeekoNo ratings yet
- Autophagy and CancerDocument349 pagesAutophagy and CancerSohibun21No ratings yet
- 2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentDocument9 pages2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentCharley WangNo ratings yet
- He367t R1 RCDocument2 pagesHe367t R1 RCSedighe VafaieNo ratings yet
- Rebekah Wilson PT ResumeDocument3 pagesRebekah Wilson PT Resumeapi-487211279No ratings yet
- Omeprazole Drug StudyDocument8 pagesOmeprazole Drug StudyJe Michelle LoayonNo ratings yet