You might also like
- Nursing Leadership and Management 2Document8 pagesNursing Leadership and Management 2Maybelyn JoradoNo ratings yet
- NICU Nursing Care PlanDocument3 pagesNICU Nursing Care Planlorence_cachoNo ratings yet
- Drug StudyDocument40 pagesDrug StudyLyka Milo AvilaNo ratings yet
- TAHBSO ReportDocument4 pagesTAHBSO ReportsachiiMeNo ratings yet
- NCP BMDocument1 pageNCP BMSourabh MehraNo ratings yet
- Guide To Making NCPDocument7 pagesGuide To Making NCPKryza Dale Bunado BaticanNo ratings yet
- HypopituitarismDocument2 pagesHypopituitarismAnne de VeraNo ratings yet
- Course in The WardDocument1 pageCourse in The WardGeevee Naganag VentulaNo ratings yet
- Impaired Gas Exchange NCPDocument3 pagesImpaired Gas Exchange NCPRomel BaliliNo ratings yet
- "My Breasts Are Sore and Tender But There Is No Milk Coming Out and Im Also in Pain Due To Uterine CrampingDocument3 pages"My Breasts Are Sore and Tender But There Is No Milk Coming Out and Im Also in Pain Due To Uterine CrampingBAGUIO CATSNo ratings yet
- Corona Virus InfographicDocument1 pageCorona Virus Infographicapi-510312435No ratings yet
- Diarrhea NCP 1Document1 pageDiarrhea NCP 1Rhence Efner Saylon50% (2)
- C. Diet Date Ordered Date Performed Date Changed General Description Indications Specific Foods Taken Client's Reaction And/or Reaction To The DietDocument35 pagesC. Diet Date Ordered Date Performed Date Changed General Description Indications Specific Foods Taken Client's Reaction And/or Reaction To The Dieteuqilegna_13No ratings yet
- BronchitisDocument129 pagesBronchitisMark Norriel CajandabNo ratings yet
- Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeDocument2 pagesTotal Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeMiar QuestNo ratings yet
- PneumoniaDocument2 pagesPneumoniaPia MedinaNo ratings yet
- Diet: Bath: ActivityDocument2 pagesDiet: Bath: ActivityKristian Karl Bautista Kiw-isNo ratings yet
- BSN Iii-A Unit Ii Skills Lab ActivityDocument2 pagesBSN Iii-A Unit Ii Skills Lab ActivityDimple Castañeto CalloNo ratings yet
- Activity IntoleranceDocument6 pagesActivity IntoleranceRaidis PangilinanNo ratings yet
- Nursing Care PlanDocument8 pagesNursing Care PlanVincent QuitorianoNo ratings yet
- Far Eastern University Nursing Care Plan Nursing Diagnosis Analysis Goals and Objectives Intervention Rationale EvaluationDocument1 pageFar Eastern University Nursing Care Plan Nursing Diagnosis Analysis Goals and Objectives Intervention Rationale EvaluationSarah CarreteroNo ratings yet
- D. Pa Tho Physiology of PneumoniaDocument4 pagesD. Pa Tho Physiology of PneumoniaBill Clinton Lamira BabanNo ratings yet
- Healthcare - Nursing Care Plan - Excess Fluid VolumeDocument4 pagesHealthcare - Nursing Care Plan - Excess Fluid VolumeBenjamin CañalitaNo ratings yet
- NCP BronchopneumoniaDocument8 pagesNCP BronchopneumoniaCrisantaCasliNo ratings yet
- Prioritize Health ProblemsDocument14 pagesPrioritize Health ProblemsKhaycee XixNo ratings yet
- Nursing Care Plan (COPD - IMBALANCE NUTRITION)Document2 pagesNursing Care Plan (COPD - IMBALANCE NUTRITION)Kathleen MartinezNo ratings yet
- Hyponatremia Algorhythm Concept MapDocument2 pagesHyponatremia Algorhythm Concept Mapnursing concept mapsNo ratings yet
- CASE STUDY 2 With RETDRM VIDEO LINK (Operaña, Ellayza)Document5 pagesCASE STUDY 2 With RETDRM VIDEO LINK (Operaña, Ellayza)OPERAñA ELLAYZA RB DECANONo ratings yet
- Understanding Biopsy ProcedureDocument5 pagesUnderstanding Biopsy ProcedureDan HizonNo ratings yet
- Ariane NCP 1Document2 pagesAriane NCP 1Kristian Ray EraulaNo ratings yet
- USC Case 04 - SinusitisDocument9 pagesUSC Case 04 - SinusitisDisti Damelia SebayangNo ratings yet
- NCP HemothoraxDocument3 pagesNCP HemothoraxMichael John F. NatividadNo ratings yet
- NCP of Endometrical CancerDocument2 pagesNCP of Endometrical CancerFrando kennethNo ratings yet
- Understanding URIs (Upper Respiratory InfectionsDocument40 pagesUnderstanding URIs (Upper Respiratory InfectionsEarl JamesNo ratings yet
- PathophysiologyDocument9 pagesPathophysiologySuzette PipoNo ratings yet
- NANDA NursingDocument13 pagesNANDA NursingWaqas Javed0% (1)
- APOLONIO, JC - Natural Theory - Thomas AquinasDocument3 pagesAPOLONIO, JC - Natural Theory - Thomas AquinasJustin ApolonioNo ratings yet
- IVs & DVs of Nursing Research StudiesDocument3 pagesIVs & DVs of Nursing Research StudiesReynard Kevin FranciscoNo ratings yet
- Case Group Work #2 CHAPTER 6 Learning Exercise 6.4 L&M 03-03-2021 SituationDocument3 pagesCase Group Work #2 CHAPTER 6 Learning Exercise 6.4 L&M 03-03-2021 SituationZunnel CortesNo ratings yet
- Nursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleDocument8 pagesNursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleTrysna Ayu SukardiNo ratings yet
- Nursing Physical AssessmentDocument5 pagesNursing Physical AssessmentApril Louise PaluganNo ratings yet
- Dysfunction at The First Stage of Labor: Prolonged Latent PhaseDocument5 pagesDysfunction at The First Stage of Labor: Prolonged Latent PhaseRam Dela PeñaNo ratings yet
- Managing Labor Pain in PregnancyDocument2 pagesManaging Labor Pain in PregnancyJACOB AQUINTEYNo ratings yet
- Post-Partum Hemorrhage Pathophysiology PaperDocument5 pagesPost-Partum Hemorrhage Pathophysiology Paperapi-399619969No ratings yet
- Power Point For The Case Study About PneumoniaDocument16 pagesPower Point For The Case Study About PneumoniaJai - Ho86% (7)
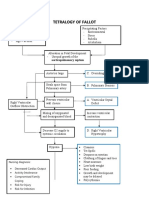
- Tetralogy of Fallot Nursing Diagnosis and ManagementDocument2 pagesTetralogy of Fallot Nursing Diagnosis and ManagementKarl KiwisNo ratings yet
- Tetralogy of Fallot Pathophysiology & Risk FactorsDocument1 pageTetralogy of Fallot Pathophysiology & Risk FactorsEiztirfNo ratings yet
- Drug StudyDocument3 pagesDrug StudyKorina FranciscoNo ratings yet
- Nursing Priority Problem List for Fluid Volume ExcessDocument1 pageNursing Priority Problem List for Fluid Volume ExcessJackyleen Kate BenetuaNo ratings yet
- The Patient and His Illness A. Pathophysiology (Book Based)Document5 pagesThe Patient and His Illness A. Pathophysiology (Book Based)Edmar Francis SabileNo ratings yet
- Choledolithiasis Cs 103 1Document34 pagesCholedolithiasis Cs 103 1Merlene Sarmiento SalungaNo ratings yet
- How to take iron supplements during pregnancyDocument7 pagesHow to take iron supplements during pregnancyjose godfreycNo ratings yet
- The Instillment of Saline in Suctioning Ebp Group DDocument46 pagesThe Instillment of Saline in Suctioning Ebp Group Dapi-340385880No ratings yet
- Instillation of Normal Saline in Endotracheal SuctioningDocument2 pagesInstillation of Normal Saline in Endotracheal SuctioningChiyouaLoverz Tharaztic JRsNo ratings yet
- Nursing 20170705 01Document4 pagesNursing 20170705 01ekaNo ratings yet
- NormalsalineinstillationbeforeendotrachealsuctioningDocument7 pagesNormalsalineinstillationbeforeendotrachealsuctioningEuis Maryah SyahidahNo ratings yet
- Continuous Positive Airway Pressure (CPAP) During The Postoperative Period For Prevention of Postoperative Morbidity and Mortality FollowinDocument4 pagesContinuous Positive Airway Pressure (CPAP) During The Postoperative Period For Prevention of Postoperative Morbidity and Mortality FollowinCharlotte ValenzuelaNo ratings yet
- Synthesis PaperDocument11 pagesSynthesis Paperapi-681331537No ratings yet
- NIV in Respiratory FailureDocument43 pagesNIV in Respiratory FailureFazil MohammedNo ratings yet
- Literature ReviewDocument11 pagesLiterature Reviewapi-340261639No ratings yet
- CHN Presentation 1Document13 pagesCHN Presentation 1api-340261639No ratings yet
- Professional DevelopmentDocument10 pagesProfessional Developmentapi-340261639No ratings yet
- Philosophy of NursingDocument1 pagePhilosophy of Nursingapi-340261639No ratings yet
- TranscriptDocument3 pagesTranscriptapi-340261639No ratings yet
- n479 Professional Activity Evaluation FormDocument3 pagesn479 Professional Activity Evaluation Formapi-340261639No ratings yet
- Nurs478 HealthcaredeliveryDocument15 pagesNurs478 Healthcaredeliveryapi-340261639No ratings yet
- Updated ResumeDocument2 pagesUpdated Resumeapi-340261639No ratings yet
- Cover Letter NursingDocument2 pagesCover Letter Nursingapi-340261639No ratings yet
- Fgi Guidelines 2014 Hop TocDocument10 pagesFgi Guidelines 2014 Hop TocZaw Moe KhineNo ratings yet
- Critical Care Nephrology Core Curriculum 2020 PDFDocument18 pagesCritical Care Nephrology Core Curriculum 2020 PDFMartín FleiNo ratings yet
- NYCM Quill + Scope - Vol 3Document102 pagesNYCM Quill + Scope - Vol 3burxardNo ratings yet
- Effectiveness of Communication Board On Level of Satisfaction Over Communication Among Mechanically Venitlated PatientsDocument6 pagesEffectiveness of Communication Board On Level of Satisfaction Over Communication Among Mechanically Venitlated PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Sofa ScoreDocument3 pagesSofa ScoreTaufik HakimNo ratings yet
- Indirect Calorimetry in Critical Illness A New.3Document10 pagesIndirect Calorimetry in Critical Illness A New.3gjk5q24qrqNo ratings yet
- Initial Fluid Resuscitation Guided by The Parkland Formula Leads T - 2023 - BurnDocument8 pagesInitial Fluid Resuscitation Guided by The Parkland Formula Leads T - 2023 - BurnBrenda Serrano LaraNo ratings yet
- Narrative ReportDocument2 pagesNarrative ReportJanina Cate D TorrecampoNo ratings yet
- Natural ResourcesDocument5 pagesNatural ResourcessandeepNo ratings yet
- Hospital ICU Organization and TypesDocument82 pagesHospital ICU Organization and TypesPaul Shan GoNo ratings yet
- 2013 Book HandbookOfHealthcareOperationsDocument541 pages2013 Book HandbookOfHealthcareOperationsabebawNo ratings yet
- 1.0 Space Standards & Dimensions: 1.1 CorridorsDocument6 pages1.0 Space Standards & Dimensions: 1.1 CorridorsMuskanNo ratings yet
- Open Heart Surgery-Post Op CareDocument6 pagesOpen Heart Surgery-Post Op CareJynrose Kaye Gulpany100% (4)
- Nursing Aide ResumeDocument2 pagesNursing Aide ResumeMayta Bacud RamosNo ratings yet
- Preventing VAPDocument8 pagesPreventing VAPyankesNo ratings yet
- End-Of-Life Care in The Icu: Supporting Nurses To Provide High-Quality CareDocument5 pagesEnd-Of-Life Care in The Icu: Supporting Nurses To Provide High-Quality CareSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- CV Alin Revisi 2016Document5 pagesCV Alin Revisi 2016Global medik indonesiaNo ratings yet
- Surving Sepsis Campaign ResultDocument8 pagesSurving Sepsis Campaign Resultmaria arenas de itaNo ratings yet
- 61 4 ATI CongresDocument38 pages61 4 ATI CongresRomaNo ratings yet
- OxigenoterapiaDocument55 pagesOxigenoterapiadanielaNo ratings yet
- Pain Assessment in The Critically Ill Adult PDFDocument11 pagesPain Assessment in The Critically Ill Adult PDFFelicia Risca RyandiniNo ratings yet
- Infection Prevention and Control Policies and Guidelines For Health Care ServicesDocument324 pagesInfection Prevention and Control Policies and Guidelines For Health Care ServicesAlejandro Caballero ChumillasNo ratings yet
- Características Clínicas y Resultados de Los Pacientes Con COVID-19 Con Ventilación Invasiva en ArgentinaDocument10 pagesCaracterísticas Clínicas y Resultados de Los Pacientes Con COVID-19 Con Ventilación Invasiva en ArgentinaSMIBA MedicinaNo ratings yet
- Predictors Post Op VentilationDocument48 pagesPredictors Post Op VentilationMuhammad Azam Mohd NizaNo ratings yet
- Test Bank For Understanding The Essentials of Critical Care Nursing 2nd Edition Kathleen Ouimet Perrin Carrie Edgerly MacleodDocument9 pagesTest Bank For Understanding The Essentials of Critical Care Nursing 2nd Edition Kathleen Ouimet Perrin Carrie Edgerly MacleodFelix Guy100% (26)
- Stiegelmeyer Sicuro Pesa Hospital Bed Brochure en V05Document7 pagesStiegelmeyer Sicuro Pesa Hospital Bed Brochure en V05Miguel GonzalezNo ratings yet
- HOSPITAL LITERATURE STUDY: KEY AREAS AND DESIGN CONSIDERATIONSDocument32 pagesHOSPITAL LITERATURE STUDY: KEY AREAS AND DESIGN CONSIDERATIONSShivanand Pegu100% (1)
- HEALTH-GROUP MEDICLAIM June 2021Document61 pagesHEALTH-GROUP MEDICLAIM June 2021Kishore mohan ManapuramNo ratings yet
- cEEG Monitoring in The ICU: Treating Subclinical Seizures Is Cost EffectiveDocument26 pagescEEG Monitoring in The ICU: Treating Subclinical Seizures Is Cost EffectiveVijay GadagiNo ratings yet
- Pressure Ulcer Assessment and Treatment (PDFDrive)Document88 pagesPressure Ulcer Assessment and Treatment (PDFDrive)Amna AliNo ratings yet