You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- HOSPITAL INSTITUSI Parameter For Hosp Performance 2012 - 2014 Update Jan 2015Document24 pagesHOSPITAL INSTITUSI Parameter For Hosp Performance 2012 - 2014 Update Jan 2015arnol3090No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- NIH Guidelines On Conducting Research in The MOHDocument2 pagesNIH Guidelines On Conducting Research in The MOHarnol3090No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Shock & Fluid TherapyDocument57 pagesShock & Fluid Therapyarnol3090No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Eye Department Queen Elizabeth HospitalDocument43 pagesEye Department Queen Elizabeth Hospitalarnol3090No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Red EyesDocument86 pagesRed Eyesarnol3090No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Types of specimens and containers for lab testsDocument1 pageTypes of specimens and containers for lab testsarnol3090No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Paediatric Ophthalmology: DR Shuaibah Ab - Ghani Paediatric Ophthalmologist Hospital Queen Elizabeth Kota KinabaluDocument41 pagesPaediatric Ophthalmology: DR Shuaibah Ab - Ghani Paediatric Ophthalmologist Hospital Queen Elizabeth Kota Kinabaluarnol3090No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Senarai Semak Code Blue BagDocument2 pagesSenarai Semak Code Blue Bagarnol3090No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Ocular Injuries and EmergenciesDocument60 pagesOcular Injuries and Emergenciesarnol3090100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Anisman Acute Vision LossDocument68 pagesAnisman Acute Vision Lossarnol3090No ratings yet
- 2010 Guidelines Instructor UpdateDocument148 pages2010 Guidelines Instructor UpdateAnastasia Citra PurwaniNo ratings yet
- GoutDocument36 pagesGoutKylie LeeNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Ventilator Settings GuideDocument7 pagesVentilator Settings Guidearnol3090No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- SOP Forensic Medicine ServicesDocument78 pagesSOP Forensic Medicine Servicesarnol3090No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Senarai Semak Troli KecemasanDocument2 pagesSenarai Semak Troli Kecemasanarnol309050% (4)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Eye Department Queen Elizabeth HospitalDocument43 pagesEye Department Queen Elizabeth Hospitalarnol3090No ratings yet
- Anisman Acute Vision LossDocument68 pagesAnisman Acute Vision Lossarnol3090No ratings yet
- Hydralazine D NepeanDocument2 pagesHydralazine D Nepeanarnol3090No ratings yet
- Management of Stable Angina PectorisDocument84 pagesManagement of Stable Angina Pectorisarnol3090No ratings yet
- Medical Assistants Registration) Act 1977Document9 pagesMedical Assistants Registration) Act 1977arnol3090No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Anatomy & Physiology of The EyeDocument22 pagesAnatomy & Physiology of The Eyearnol3090No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Ocular Injuries and EmergenciesDocument60 pagesOcular Injuries and Emergenciesarnol3090100% (1)
- Neonatal TSH ELISA Screening TestDocument10 pagesNeonatal TSH ELISA Screening Testyandros666No ratings yet
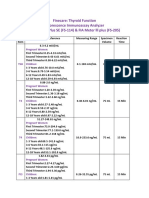
- Thyroid FunctionDocument2 pagesThyroid FunctionSm Bikash Kumar MohonNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Protraction Facial Mask Corrects Midfacial RetrusionDocument7 pagesProtraction Facial Mask Corrects Midfacial RetrusionMaria-Lavinia HoinaruNo ratings yet
- Douglas Stanley On The Jaw & MouthDocument12 pagesDouglas Stanley On The Jaw & MouthNick Enriquez SchollNo ratings yet
- Vertigo Due To Vascular MechanismsDocument9 pagesVertigo Due To Vascular Mechanismsrafael rocha novaesNo ratings yet
- Haytham's - Final - FileDocument229 pagesHaytham's - Final - FileFredrik OlsenNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- At The Dentist's - Vocabulary and WordsearchDocument4 pagesAt The Dentist's - Vocabulary and WordsearchĽubomírNo ratings yet
- The TracheaDocument16 pagesThe TracheaMatende husseinNo ratings yet
- Comprehensive Review in Clinical Neurology - A Multiple Choice Question BookDocument1,507 pagesComprehensive Review in Clinical Neurology - A Multiple Choice Question Bookcassiolacerda100% (18)
- Anatomy of EarDocument27 pagesAnatomy of EarKhush BakhtNo ratings yet
- Head and Neck Surgery Anatomy and Thyroid NeoplasmsDocument92 pagesHead and Neck Surgery Anatomy and Thyroid NeoplasmsAlbert GheorgheNo ratings yet
- Classification of MalocclusionDocument30 pagesClassification of MalocclusionMohamed FarahatNo ratings yet
- Temporal Bone Dissection - The ZURICH GuidelinesDocument66 pagesTemporal Bone Dissection - The ZURICH GuidelinesAhmed Morsy0% (1)
- McqsDocument1 pageMcqssimitsherinNo ratings yet
- Anatomy and Physiology THT - Dr. AriefDocument88 pagesAnatomy and Physiology THT - Dr. AriefGilbert Sterling OctaviusNo ratings yet
- Esthetics in Dental ImplantsDocument87 pagesEsthetics in Dental ImplantsRavi Uttara100% (3)
- The Homeopathic Treatment of Ear InfectionsDocument104 pagesThe Homeopathic Treatment of Ear Infectionsdipgang7174No ratings yet
- Kode Icd 10Document29 pagesKode Icd 10Zakia NisakNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pathogenesis of Hearing Loss ExplainedDocument6 pagesPathogenesis of Hearing Loss ExplainedYogi HadityaNo ratings yet
- Basic of Ophthalmology ExaminationsDocument47 pagesBasic of Ophthalmology ExaminationsAnonymous iy7I3o100% (2)
- Muscles of Mastication Sumana SeminarDocument68 pagesMuscles of Mastication Sumana SeminarSumana AryaNo ratings yet
- Nerves and Vessels of the OrbitDocument27 pagesNerves and Vessels of the OrbitFadli LatamaNo ratings yet
- AOMSI Calender of Events 2024 FinalDocument4 pagesAOMSI Calender of Events 2024 FinalsevattapillaiNo ratings yet
- Trigeminal Nerve Seminar on Applied AnatomyDocument37 pagesTrigeminal Nerve Seminar on Applied AnatomyMAYANK MITTALNo ratings yet
- Shivani Lab ReportDocument2 pagesShivani Lab ReportJames MooreNo ratings yet
- Orthodontic AssessmentDocument30 pagesOrthodontic Assessmentmentacity10100% (2)
- TF TestDocument23 pagesTF TestFrederick BallesterosNo ratings yet
- Frog Nervous SystemDocument24 pagesFrog Nervous SystemBeaNo ratings yet
- Leukodystrophies ImagingDocument27 pagesLeukodystrophies ImagingPartha GanesanNo ratings yet
- Thyroid Nodules and GoiterDocument7 pagesThyroid Nodules and GoiterAgustinaNo ratings yet