You might also like
- Atopic DermatitisDocument9 pagesAtopic DermatitisJorge De VeraNo ratings yet
- Measuring and Describing MotionDocument22 pagesMeasuring and Describing MotionRenz Dela Cruz ArellanoNo ratings yet
- Coriolis EffectDocument18 pagesCoriolis Effectletter_ashish4444No ratings yet
- Salas v. First Finance Leasing CorporationDocument2 pagesSalas v. First Finance Leasing CorporationKatrina PerezNo ratings yet
- Final Examination: Polytechnic University of The Philippines Open Universitysysten4Document1 pageFinal Examination: Polytechnic University of The Philippines Open Universitysysten4Leigh LynNo ratings yet
- Dy Pac v. Bataan Replevin CaseDocument2 pagesDy Pac v. Bataan Replevin Caseanalyn100% (1)
- Ecuadors Restrictive Abortion Laws and Public HealthDocument21 pagesEcuadors Restrictive Abortion Laws and Public Healthangluna89No ratings yet
- Synthesis of Banana Flavor Isoamyl AcetateDocument12 pagesSynthesis of Banana Flavor Isoamyl AcetatePatricia HariramaniNo ratings yet
- Chapter 9 Answer KeyDocument34 pagesChapter 9 Answer KeyFirebirdGT50% (2)
- Phylum RhizopodaDocument2 pagesPhylum RhizopodaLiborMyslivecek100% (1)
- Public Speaking Materials and TipsDocument2 pagesPublic Speaking Materials and Tipsstrawberry_89No ratings yet
- Agad V MabatoDocument3 pagesAgad V MabatoHudson CeeNo ratings yet
- Quiz 07Document11 pagesQuiz 07sullivan583No ratings yet
- Quiz 9Document189 pagesQuiz 9Joshua PayneNo ratings yet
- The Carnot cycle explainedDocument3 pagesThe Carnot cycle explainedwaqas_730_2006No ratings yet
- Croup SyndromeDocument3 pagesCroup SyndromeMabesNo ratings yet
- Applied Ethics Abortion: 1. Abortion Is An "Act Which A Woman Performs in Voluntarily Terminating, orDocument8 pagesApplied Ethics Abortion: 1. Abortion Is An "Act Which A Woman Performs in Voluntarily Terminating, oryip90No ratings yet
- Thermodynamics Rankine ExamplesDocument8 pagesThermodynamics Rankine ExamplesSre VinodNo ratings yet
- Treating Atopic Dermatitis in Children Under 40 CharactersDocument26 pagesTreating Atopic Dermatitis in Children Under 40 CharactersAnnisa SasaNo ratings yet
- Bank Liable for Forgery Despite Contributory NegligenceDocument13 pagesBank Liable for Forgery Despite Contributory NegligenceKirby ReniaNo ratings yet
- 3 - Parties - Dela Cruz Vs Joaquin, G.R. No. 162788. July 28, 2005Document2 pages3 - Parties - Dela Cruz Vs Joaquin, G.R. No. 162788. July 28, 2005Mary Grace Baynosa-CoNo ratings yet
- Nanda Nursing Diagnosis Examples:: Vague Uneasy Feeling ofDocument3 pagesNanda Nursing Diagnosis Examples:: Vague Uneasy Feeling ofYOLANDA P. DELCASTILLONo ratings yet
- Case Study AsthmaDocument11 pagesCase Study AsthmaJaya ShriNo ratings yet
- (PHY) 3.02A ElectrocardiogramDocument10 pages(PHY) 3.02A ElectrocardiogramMarilou de GuzmanNo ratings yet
- Rule 1 BJMP Rule BookDocument2 pagesRule 1 BJMP Rule BookRudy OrteaNo ratings yet
- Pyloric StenosisDocument11 pagesPyloric StenosisJustin CharlesNo ratings yet
- Debate On Abortion: A Feminist Argument: L. Bishwanth SharmaDocument6 pagesDebate On Abortion: A Feminist Argument: L. Bishwanth SharmaImpact JournalsNo ratings yet
- Acceleration in MechanismsDocument22 pagesAcceleration in Mechanismsadilshahzad2001100% (2)
- Skin Barrier Disruption and Filaggrin Mutation PathophysiologyDocument3 pagesSkin Barrier Disruption and Filaggrin Mutation PathophysiologyBanni Aprilita PratiwiNo ratings yet
- Rubrics For PosterDocument2 pagesRubrics For Posterapi-310947658No ratings yet
- Common Pediatric Fractures: Allyson S. Howe, MD Maj, Usaf, MCDocument67 pagesCommon Pediatric Fractures: Allyson S. Howe, MD Maj, Usaf, MCPrince EdwardNo ratings yet
- Abdomen ExaminationDocument37 pagesAbdomen ExaminationJaaydevNo ratings yet
- Head and Neck ExaminationDocument25 pagesHead and Neck ExaminationDarryl Betts100% (1)
- Neutrophils and Asthma: J MonteseirínDocument15 pagesNeutrophils and Asthma: J MonteseirínRupa2811No ratings yet
- BASIC ACCO Simulated MidtermDocument10 pagesBASIC ACCO Simulated MidtermistepNo ratings yet
- Angeles Vs Secretary of JusticeDocument1 pageAngeles Vs Secretary of JusticemalcolveNo ratings yet
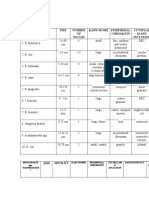
- Table 1: Protozoans Spp. "CYSTS" Size Number OF Nuclei Karyosome Peripheral Chromatin Cytoplas M and InclusionDocument3 pagesTable 1: Protozoans Spp. "CYSTS" Size Number OF Nuclei Karyosome Peripheral Chromatin Cytoplas M and InclusionJoshua TrinidadNo ratings yet
- Pressure Ulcers Ecourse: Module 3 - Quiz IDocument10 pagesPressure Ulcers Ecourse: Module 3 - Quiz IjuanitoNo ratings yet
- Extra Materials Carnot EngineDocument21 pagesExtra Materials Carnot Enginetruffelove100% (1)
- Abortion and Moral CharacterDocument13 pagesAbortion and Moral CharacterCheabu Ngmenlanaa BenNo ratings yet
- Atopic Dermatitis: An Inflammatory Skin DisorderDocument22 pagesAtopic Dermatitis: An Inflammatory Skin DisorderBonitavanyNo ratings yet
- RRLDocument96 pagesRRLKristiene Kyle AquinoNo ratings yet
- Hows of UsDocument1 pageHows of UsMegan CastroNo ratings yet
- ILA - Hirschsprungs DiseaseDocument48 pagesILA - Hirschsprungs DiseaseSoleh Ramly100% (1)
- Nose and Paranasal SinusesDocument4 pagesNose and Paranasal SinusesAlloiBialbaNo ratings yet
- Abdominal Wall DefectsDocument14 pagesAbdominal Wall Defectsskeebs23No ratings yet
- Cardiovascular DisordersDocument58 pagesCardiovascular Disordersehjing100% (3)
- Republic V Bacolod Murcia DigestsDocument2 pagesRepublic V Bacolod Murcia Digestspinkblush717No ratings yet
- 5 Jose Moreno Vs Rene KhanDocument5 pages5 Jose Moreno Vs Rene KhanjovifactorNo ratings yet
- Navarro Vs Laguna Dev't Bank (398 SCRA 227, 27 February 2003)Document8 pagesNavarro Vs Laguna Dev't Bank (398 SCRA 227, 27 February 2003)Archibald Jose Tiago ManansalaNo ratings yet
- Where Does Human Life BeginDocument30 pagesWhere Does Human Life BeginAries OrtegaNo ratings yet
- HI Classmates!!!Document36 pagesHI Classmates!!!Alex SilvanoNo ratings yet
- OSG Vs. Ayala Land Ruling on Parking FeesDocument6 pagesOSG Vs. Ayala Land Ruling on Parking FeesgmcamaymayanNo ratings yet
- Evangelium VitaeDocument28 pagesEvangelium VitaeTobiasNo ratings yet
- Anp2001 Skin Quiz PDFDocument19 pagesAnp2001 Skin Quiz PDFJerilee SoCute WattsNo ratings yet
- Persuasive Essay Organ DonationDocument4 pagesPersuasive Essay Organ Donationapi-242930262No ratings yet
- Cardiac Diseases in ChildrenDocument66 pagesCardiac Diseases in ChildrenHarmas Novryan FarezaNo ratings yet
- Odia Tetralogy of FallotDocument25 pagesOdia Tetralogy of Fallotvictorjonathan567No ratings yet
- Congenital Heart DiseasesDocument14 pagesCongenital Heart DiseasesEulane Ferrer100% (1)
- Penyakit Jantung KongenitalDocument30 pagesPenyakit Jantung KongenitalrintiikNo ratings yet
- 0 18yrs Child Combined ScheduleDocument6 pages0 18yrs Child Combined ScheduleAwal Safar MNo ratings yet
- HESIDocument29 pagesHESIJustin Bunn100% (18)
- 0 18yrs Child Combined ScheduleDocument6 pages0 18yrs Child Combined ScheduleAwal Safar MNo ratings yet
- London Final Ch38Document29 pagesLondon Final Ch38Pye Antwan DelvaNo ratings yet
- Nur2310 GFT 2016-1ref 8855Document8 pagesNur2310 GFT 2016-1ref 8855Pye Antwan DelvaNo ratings yet
- Critical Thinking AckleyDocument59 pagesCritical Thinking AckleyPye Antwan DelvaNo ratings yet
- EENT Disorders StudentsDocument26 pagesEENT Disorders StudentsPye Antwan DelvaNo ratings yet
- Math Practice QuestionsDocument1 pageMath Practice QuestionsPye Antwan DelvaNo ratings yet
- Triple TDocument1 pageTriple TPye Antwan DelvaNo ratings yet
- Microscope Review GuideDocument34 pagesMicroscope Review GuideWwwanand111100% (1)
- Chapt12 LectureDocument197 pagesChapt12 LecturePye Antwan DelvaNo ratings yet
- Gi PPTDocument17 pagesGi PPTPye Antwan DelvaNo ratings yet
- Chapt02 LectureDocument163 pagesChapt02 LecturePye Antwan DelvaNo ratings yet
- AnatomyDocument90 pagesAnatomyPye Antwan DelvaNo ratings yet
- Gu PPTDocument32 pagesGu PPTPye Antwan DelvaNo ratings yet
- Nur1141 Hesi Review 3Document10 pagesNur1141 Hesi Review 3Pye Antwan DelvaNo ratings yet
- CH 29 - Management of Patients With Structural, Infectious, and Inflmmatory Cardiac DisordersDocument15 pagesCH 29 - Management of Patients With Structural, Infectious, and Inflmmatory Cardiac DisordersPye Antwan Delva100% (1)
- CH 29 - Management of Patients With Structural, Infectious, and Inflmmatory Cardiac DisordersDocument15 pagesCH 29 - Management of Patients With Structural, Infectious, and Inflmmatory Cardiac DisordersPye Antwan Delva100% (1)
- Common Drug Stems Cheat SheetDocument2 pagesCommon Drug Stems Cheat SheetCharis Mae DimaculanganNo ratings yet
- Drugs For Men's Health and Reproductive Disorders Ch57 (Student)Document20 pagesDrugs For Men's Health and Reproductive Disorders Ch57 (Student)Pye Antwan DelvaNo ratings yet
- PC Pro - October 2016 UKDocument132 pagesPC Pro - October 2016 UKPye Antwan DelvaNo ratings yet
- CH 64 - Management of Patients With Neurologic Infections, Autoimmune Disorders, and NeuropathiesDocument14 pagesCH 64 - Management of Patients With Neurologic Infections, Autoimmune Disorders, and NeuropathiesPye Antwan DelvaNo ratings yet
- CH 31 - Assessment and Management of Patients With Vascular Disorders and Problems of PeripheralDocument16 pagesCH 31 - Assessment and Management of Patients With Vascular Disorders and Problems of PeripheralPye Antwan DelvaNo ratings yet
- CIHA ch26Document14 pagesCIHA ch26Pye Antwan DelvaNo ratings yet
- Indications: PurposeDocument13 pagesIndications: PurposeIRA ODETTE GATUSNo ratings yet
- Essential Newborn Care: Fluid (Green Amniotic Fluid) ) To Prevent AspirationDocument17 pagesEssential Newborn Care: Fluid (Green Amniotic Fluid) ) To Prevent AspirationthadzamingNo ratings yet
- (Harsh Mohan) Textbook of Pathology (6th Ed.) - 433-476Document44 pages(Harsh Mohan) Textbook of Pathology (6th Ed.) - 433-476Ananta DasNo ratings yet
- Classification of Congenital Heart DiseasesDocument16 pagesClassification of Congenital Heart DiseasesdoctorriyasNo ratings yet
- Preox Reox Article PDFDocument7 pagesPreox Reox Article PDFTaha OpedNo ratings yet
- Oxygen Insufficiency.Document54 pagesOxygen Insufficiency.Josephine George JojoNo ratings yet
- Di V V: Cardiomath Equations InfoDocument35 pagesDi V V: Cardiomath Equations InfoMd. ashfaque Ahemmed khanNo ratings yet
- Congenital Heart DiseaseDocument93 pagesCongenital Heart DiseaseManjunatha HR100% (1)
- Identifying Newborns With Critical Congenital Heart DiseaseDocument32 pagesIdentifying Newborns With Critical Congenital Heart DiseaseHardian RakhmawardanaNo ratings yet
- Congenital Heart Disease: Education and Practice GapsDocument18 pagesCongenital Heart Disease: Education and Practice GapsAlvaro Ignacio Lagos SuilNo ratings yet
- CARDIAC CATHETERIZATION LABORATORY AN INTRODUCTORY MANUAL, University of TennesseeDocument29 pagesCARDIAC CATHETERIZATION LABORATORY AN INTRODUCTORY MANUAL, University of TennesseeNavojit ChowdhuryNo ratings yet
- Left To Right Shunt Congenital Heart Disease As A Risk Factor of Recurrent Pneumonia in Under Five-Year-Old Children - A Single Centre Experience in Bandung IndonesiaDocument5 pagesLeft To Right Shunt Congenital Heart Disease As A Risk Factor of Recurrent Pneumonia in Under Five-Year-Old Children - A Single Centre Experience in Bandung IndonesiaAndrewNo ratings yet
- (PED) 1.03a Neonatal Assessment Part 1 - Salazar (v2)Document21 pages(PED) 1.03a Neonatal Assessment Part 1 - Salazar (v2)RL MarquezNo ratings yet
- Best Management in Isolated Right Ventricular Hypoplasia With Septal Defects in AdultsDocument7 pagesBest Management in Isolated Right Ventricular Hypoplasia With Septal Defects in AdultsReinaldi octaNo ratings yet
- Acyanotic Congenital Heart Disease: Left-to-Right Shunt LesionsDocument17 pagesAcyanotic Congenital Heart Disease: Left-to-Right Shunt LesionsAgustinaNo ratings yet
- Understanding Cardiac ShuntsDocument10 pagesUnderstanding Cardiac ShuntsDani GodoyNo ratings yet
- Cardiac Surgery MCQDocument43 pagesCardiac Surgery MCQprofarmah100% (7)
- Cardiovascular Patho 1 OgenaDocument87 pagesCardiovascular Patho 1 OgenaQuolette ConstanteNo ratings yet
- Ecocardiografia NeonatalDocument10 pagesEcocardiografia NeonatalRonald MHNo ratings yet
- Assessing Operability of Congenital Heart Defects With Elevated Pulmonary Vascular ResistanceDocument6 pagesAssessing Operability of Congenital Heart Defects With Elevated Pulmonary Vascular ResistancedeepaNo ratings yet
- Fetal CirculationDocument2 pagesFetal Circulationanon_414797925No ratings yet
- Detecting Heartbeats and Diagnosing Chest PainDocument113 pagesDetecting Heartbeats and Diagnosing Chest PainNasan Shehada100% (1)
- Anomalous Pulmonary Venous Drainage: A Pictorial Essay With A CT FocusDocument13 pagesAnomalous Pulmonary Venous Drainage: A Pictorial Essay With A CT FocusIchel Silva FndzNo ratings yet
- PdaDocument43 pagesPdaSandy ShahNo ratings yet
- NEWBORN ASSESSMENT DajuuuuuuuuuuuuuuuuDocument31 pagesNEWBORN ASSESSMENT Dajuuuuuuuuuuuuuuuuamal abdulrahmanNo ratings yet
- Final Examination in Radiology2015Document13 pagesFinal Examination in Radiology2015Ndor BariboloNo ratings yet
- Superior Vena Cava Flow 2020Document6 pagesSuperior Vena Cava Flow 2020Betül DUMANNo ratings yet
- CV-Prof-MulyadiDocument69 pagesCV-Prof-MulyadityesNo ratings yet
- Pathophysiology and Natural History of Atrial Septal DefectDocument10 pagesPathophysiology and Natural History of Atrial Septal DefectrosaNo ratings yet
- EisenmengerDocument5 pagesEisenmengerEl loco CNo ratings yet