You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Code of Ethics For Professional TeachersDocument4 pagesCode of Ethics For Professional Teachersnhengjr50% (2)
- Katz IndexDocument2 pagesKatz IndexnhengjrNo ratings yet
- Elementary Math CompetenciesDocument22 pagesElementary Math CompetenciesDianne Atting-DiazNo ratings yet
- Infant Care and Feeding TopicsDocument1 pageInfant Care and Feeding TopicsnhengjrNo ratings yet
- General Survey: Nelly Jr. C. Freyra-Ombao, RN, MDDocument33 pagesGeneral Survey: Nelly Jr. C. Freyra-Ombao, RN, MDnhengjrNo ratings yet
- Katz IndexDocument2 pagesKatz IndexnhengjrNo ratings yet
- Mitchella Partridge Berry Materia Medica HerbsDocument3 pagesMitchella Partridge Berry Materia Medica HerbsAlejandra GuerreroNo ratings yet
- RADIATION SAFETY FUNDAMENTALSDocument69 pagesRADIATION SAFETY FUNDAMENTALSJay Lawson100% (1)
- Physics SyllabusDocument85 pagesPhysics Syllabusalex demskoyNo ratings yet
- Module 37 Nur 145Document38 pagesModule 37 Nur 145Marga WreatheNo ratings yet
- Binge-Eating Disorder in AdultsDocument19 pagesBinge-Eating Disorder in AdultsJaimeErGañanNo ratings yet
- Regenerative Medicine Manual ISSCA 2020 EnglishDocument21 pagesRegenerative Medicine Manual ISSCA 2020 EnglishDana MihutNo ratings yet
- Cars Ger Eu PCDocument157 pagesCars Ger Eu PCsergeyNo ratings yet
- Electrical Units of MeasureDocument36 pagesElectrical Units of MeasureHyung BaeNo ratings yet
- 366 Community Service IdeasDocument5 pages366 Community Service IdeasAhmetYılmazVuralNo ratings yet
- Desiderata: by Max EhrmannDocument6 pagesDesiderata: by Max EhrmannTanay AshwathNo ratings yet
- Lectura Isaac NewtonDocument2 pagesLectura Isaac NewtonCESAR MAURICIO RODRIGUEZNo ratings yet
- GE - Oil Sheen Detection, An Alternative To On-Line PPM AnalyzersDocument2 pagesGE - Oil Sheen Detection, An Alternative To On-Line PPM AnalyzersjorgegppNo ratings yet
- LOD Spec 2016 Part I 2016-10-19 PDFDocument207 pagesLOD Spec 2016 Part I 2016-10-19 PDFzakariazulkifli92No ratings yet
- Forecasting ExercisesDocument2 pagesForecasting ExercisesAsh VinaNo ratings yet
- MPC-006 DDocument14 pagesMPC-006 DRIYA SINGHNo ratings yet
- Takara 2012Document57 pagesTakara 2012Deepak Ranjan SahooNo ratings yet
- UPSC IFS Botany Syllabus: Paper - IDocument3 pagesUPSC IFS Botany Syllabus: Paper - IVikram Singh ChauhanNo ratings yet
- Elements of Plane and Spherical Trigonometry With Numerous Practical Problems - Horatio N. RobinsonDocument228 pagesElements of Plane and Spherical Trigonometry With Numerous Practical Problems - Horatio N. RobinsonjorgeNo ratings yet
- Lesson 1 - Simple StressDocument5 pagesLesson 1 - Simple StressJohn Philip NadalNo ratings yet
- Gps Vehicle Tracking System ProjectDocument3 pagesGps Vehicle Tracking System ProjectKathrynNo ratings yet
- Ampersand MenuDocument5 pagesAmpersand MenuJozefNo ratings yet
- The Baptismal Liturgy in The Easter Vigil According To The Sacramentary of Fulda (10th Century)Document7 pagesThe Baptismal Liturgy in The Easter Vigil According To The Sacramentary of Fulda (10th Century)Henry DonascoNo ratings yet
- 19 - Speed, Velocity and Acceleration (Answers)Document4 pages19 - Speed, Velocity and Acceleration (Answers)keyur.gala100% (1)
- DGPS Sensor JLR-4331W Instruction ManualDocument42 pagesDGPS Sensor JLR-4331W Instruction ManualantonioNo ratings yet
- Vincent Hoa's English 101 PortfolioDocument24 pagesVincent Hoa's English 101 PortfoliovincentNo ratings yet
- White Paper Without Track ChangesDocument7 pagesWhite Paper Without Track Changesapi-609064761No ratings yet
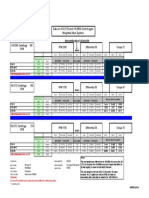
- HS-2172 Vs HS-5500 Test ComparisonDocument1 pageHS-2172 Vs HS-5500 Test ComparisonRicardo VillarNo ratings yet
- Palm Wine SpecificationDocument10 pagesPalm Wine SpecificationUday ChaudhariNo ratings yet
- Chapter 7 (Additional Notes) Thermodynamics Review (Power Plant Technology by M Wakil)Document29 pagesChapter 7 (Additional Notes) Thermodynamics Review (Power Plant Technology by M Wakil)Aries SattiNo ratings yet
- ATEX Certified FiltersDocument4 pagesATEX Certified FiltersMarco LoiaNo ratings yet