You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Review of Systems TemplateDocument1 pageReview of Systems TemplateJessica Nishikawa84% (37)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Bedside Medicine Without Tears Chugh PDFDocument454 pagesBedside Medicine Without Tears Chugh PDFAishwaray KohliNo ratings yet
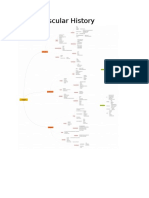
- Cardiovascular History MindmapDocument12 pagesCardiovascular History MindmapThe_BakerNo ratings yet
- Differential Diagnosis of Common Presenting ComplaintsDocument4 pagesDifferential Diagnosis of Common Presenting ComplaintsPebblesNo ratings yet
- Copd Case StudyDocument6 pagesCopd Case StudyDivine ParagasNo ratings yet
- EnglishDocument15 pagesEnglishSussel Escribas ValeroNo ratings yet
- ASTHMADocument16 pagesASTHMASussel Escribas ValeroNo ratings yet
- ASTHMADocument16 pagesASTHMASussel Escribas ValeroNo ratings yet
- Color Blind EssentialsDocument28 pagesColor Blind EssentialsNatria Adek KeciikNo ratings yet
- Asthma Fullguideline 2009Document132 pagesAsthma Fullguideline 2009Lajwanti DesignersNo ratings yet
- Askep Ppok - Kelompok 1Document17 pagesAskep Ppok - Kelompok 1super manggis100% (1)
- Edmunds: Introduction To Clinical Pharmacology, 8th Edition: Answer Keys - in Text Critical Thinking QuestionsDocument38 pagesEdmunds: Introduction To Clinical Pharmacology, 8th Edition: Answer Keys - in Text Critical Thinking QuestionsAnnaNo ratings yet
- Ambra GriesaDocument31 pagesAmbra GriesaShubhanshi Bhasin100% (2)
- Aerosol Medications For Treatment of Mucus Clearance DisordersDocument8 pagesAerosol Medications For Treatment of Mucus Clearance DisordersT M Santhosh KumarNo ratings yet
- Basic Principles in Occupational Hygiene (Student Manual)Document206 pagesBasic Principles in Occupational Hygiene (Student Manual)Kim Myers100% (7)
- Pharma GermaniaDocument10 pagesPharma GermaniaTeboho MokhesengNo ratings yet
- PediatricsDocument3 pagesPediatricsTheju ReddyNo ratings yet
- Cough: 4 Phases of Cough ReflexDocument4 pagesCough: 4 Phases of Cough ReflexNadhirah ZulkifliNo ratings yet
- Ascoril Expectorant - FAQ'sDocument16 pagesAscoril Expectorant - FAQ'skurutalaNo ratings yet
- Nurse Deployment Program NDP Examination NotesDocument44 pagesNurse Deployment Program NDP Examination NotesAngelo Quixote100% (1)
- المسار غير الجراحيDocument21 pagesالمسار غير الجراحيAhmad L YasinNo ratings yet
- Respirology 2023 FinalDocument127 pagesRespirology 2023 FinalBelinda ELISHANo ratings yet
- Oil Pulling Universal RemedyDocument15 pagesOil Pulling Universal RemedyAtma Love100% (1)
- Ambroxol PDFDocument2 pagesAmbroxol PDFmina zayNo ratings yet
- A Guide To Your: COVID-19 VaccinationDocument8 pagesA Guide To Your: COVID-19 Vaccinationalinaluca30No ratings yet
- Ailment ReflectionsDocument3 pagesAilment ReflectionsAdnan AhmedNo ratings yet
- (2011!06!29) CMED The Medical Writeup HandoutDocument19 pages(2011!06!29) CMED The Medical Writeup HandoutAdel TaradjiNo ratings yet
- Stridor, Aspiration, and Cough in ChildrenDocument41 pagesStridor, Aspiration, and Cough in ChildrenArif Rahman DmNo ratings yet
- Materia-Medica of Nosods by AllenDocument590 pagesMateria-Medica of Nosods by AllenG AnshuNo ratings yet
- Drugs Acting On Respiratory System of AnimalsDocument8 pagesDrugs Acting On Respiratory System of AnimalsSunil100% (4)
- NCP and Prioritization For PneumoniaDocument6 pagesNCP and Prioritization For PneumoniaLawrence AzicateNo ratings yet
- A Comprehensive Acupuncture Points Database: By: Shmuel Halevi PH.DDocument38 pagesA Comprehensive Acupuncture Points Database: By: Shmuel Halevi PH.DPraveen Kumar100% (1)
- Content On Pediatric Asthma: Submitted To Mrs. Rupinder Kaur Lecturer Submitted by Anu George MSC Nsg. 1 YearDocument11 pagesContent On Pediatric Asthma: Submitted To Mrs. Rupinder Kaur Lecturer Submitted by Anu George MSC Nsg. 1 YeargopscharanNo ratings yet
- The Case History Scheme: Kyiv State Hospital Pediatric Department 1Document8 pagesThe Case History Scheme: Kyiv State Hospital Pediatric Department 1Fatemeh BemanaNo ratings yet