You might also like
- Chapter 6: PHARDOSEDocument6 pagesChapter 6: PHARDOSEAlyssa Marie L. Palamiano100% (1)
- Pharmaceutical Care Plan and Documentaion of Pharmacotherapy Intervention (MTM)Document67 pagesPharmaceutical Care Plan and Documentaion of Pharmacotherapy Intervention (MTM)CAROL ANN PATITICONo ratings yet
- Aetna 1850 HD PlanDocument10 pagesAetna 1850 HD PlanNaveen ChintamaniNo ratings yet
- Pre-Reg CalculationsDocument58 pagesPre-Reg Calculationsm886100% (1)
- RA 3720 Vs RA 9711Document7 pagesRA 3720 Vs RA 9711lem86% (7)
- Pharmaceutical CareDocument114 pagesPharmaceutical CareRisdaFitriaNo ratings yet
- Pharmaceutical SOP ExampleDocument4 pagesPharmaceutical SOP ExampleFaysal AhmedNo ratings yet
- Clinical PharmacistDocument2 pagesClinical PharmacistArif Ali RphNo ratings yet
- Dr. Ruth NamyaloDocument62 pagesDr. Ruth NamyaloHarun MohamedNo ratings yet
- Pharm Care 4 Chapter 1Document25 pagesPharm Care 4 Chapter 1MaraNagaSambarani100% (1)
- Selective Pain Reliever Acting in CNS or PeripheryDocument42 pagesSelective Pain Reliever Acting in CNS or PeripheryVinayak SinghNo ratings yet
- Medication Error 7Document20 pagesMedication Error 7Riduwan BamahfudNo ratings yet
- Medication Therapy ManagementDocument20 pagesMedication Therapy ManagementAman UpadhyayNo ratings yet
- Final Hospital Pharmacy Module 3Document10 pagesFinal Hospital Pharmacy Module 3Meryl Ann Ibarra-InganNo ratings yet
- 2013 Introduction of Clinical PharmacyDocument18 pages2013 Introduction of Clinical Pharmacyyudi100% (1)
- Application of PK in Clinical SitutionDocument42 pagesApplication of PK in Clinical Situtionsafia mehmood100% (1)
- 3B - Clinical PharmacyDocument35 pages3B - Clinical PharmacyekramNo ratings yet
- Optimizing Patient Care Through Clinical PharmacyDocument14 pagesOptimizing Patient Care Through Clinical Pharmacydaniya nadeem100% (1)
- Clinical Physiology and Pharmacology: The EssentialsFrom EverandClinical Physiology and Pharmacology: The EssentialsRating: 4 out of 5 stars4/5 (1)
- Farmakoepidemiologi 2018 UmmDocument23 pagesFarmakoepidemiologi 2018 UmmSeptiani Ayu100% (1)
- SBARDocument2 pagesSBARJason Kai Poth100% (1)
- Farmakoterapi Pada LansiaDocument29 pagesFarmakoterapi Pada LansiaPuterinugraha Wanca ApatyaNo ratings yet
- M.Pharm - Hospital & Clinical PharmacyDocument11 pagesM.Pharm - Hospital & Clinical PharmacyMohan VarmaNo ratings yet
- Clinical Pharmacy in Pediatric NephrologyDocument34 pagesClinical Pharmacy in Pediatric NephrologyAta07No ratings yet
- Pharmacy Pharm DDocument97 pagesPharmacy Pharm DDeepa SruthiNo ratings yet
- Hospital PharmacyDocument13 pagesHospital PharmacySridivya SrihariNo ratings yet
- Analisis Pengelolaan Obat Di Puskesmas Kampala Kecamatan Sinjai PDFDocument10 pagesAnalisis Pengelolaan Obat Di Puskesmas Kampala Kecamatan Sinjai PDFPradika Nudya Risalati RachmanNo ratings yet
- Introduction PC 2017Document20 pagesIntroduction PC 2017ChristinaNo ratings yet
- Leaflet TBCDocument2 pagesLeaflet TBCircakoeNo ratings yet
- Pharmaceutical CareDocument27 pagesPharmaceutical Caremai elewaNo ratings yet
- Pharmacokinetic Drug Interactions: Syed Imran Prof. Mrs. Vidya. P. SableDocument20 pagesPharmacokinetic Drug Interactions: Syed Imran Prof. Mrs. Vidya. P. SableDALI SAPARI 2021No ratings yet
- Compartmental ModelDocument5 pagesCompartmental ModelIlyax KahnNo ratings yet
- Floating Drug Delivery SystemDocument27 pagesFloating Drug Delivery SystemGANESH KUMAR JELLA100% (1)
- Drug Utilization ReviewsDocument7 pagesDrug Utilization ReviewsenoyNo ratings yet
- European Society of Clinical Pharmacy (ESCP) Copenhagen 2014Document37 pagesEuropean Society of Clinical Pharmacy (ESCP) Copenhagen 2014happyscottlee3438No ratings yet
- Ward Round Participation Benefits for PharmacistsDocument2 pagesWard Round Participation Benefits for PharmacistsAnonymous whcvnPBeQNo ratings yet
- Computational Modeling of Drug DispositionDocument1 pageComputational Modeling of Drug DispositionVaishali PathakNo ratings yet
- Drug Related Problem Dan SOAP WordDocument18 pagesDrug Related Problem Dan SOAP WordIflakhatul UlfaNo ratings yet
- Pharmaco EpidemiologyDocument3 pagesPharmaco EpidemiologyAnne RajeshNo ratings yet
- Rational Use of Drugs-IDocument38 pagesRational Use of Drugs-IUmair Mazhar100% (1)
- Self-Medication (PSBH Project 2010)Document54 pagesSelf-Medication (PSBH Project 2010)Varun Shah100% (1)
- Hospital PharmacyDocument32 pagesHospital Pharmacyenterprenuer celNo ratings yet
- Medication Adherence Scale PDFDocument13 pagesMedication Adherence Scale PDFRommel G. SantiagoNo ratings yet
- Drug Utilization Study (Dus)Document17 pagesDrug Utilization Study (Dus)Arif Budiman100% (1)
- Kit System ManagementDocument29 pagesKit System ManagementTifa IstiwaNo ratings yet
- Pharmaceutical Care Process Overview PDFDocument2 pagesPharmaceutical Care Process Overview PDFWawan KurniawanNo ratings yet
- Pharmaceutical Care ConceptDocument38 pagesPharmaceutical Care ConceptTiti SulistiowatiNo ratings yet
- Apollojames Lecturer Nandha College of PharmacyDocument19 pagesApollojames Lecturer Nandha College of PharmacySuresh ThanneruNo ratings yet
- Drug Administration Through An Enteral Feeding.27Document9 pagesDrug Administration Through An Enteral Feeding.27Kayo Alves FigueiredoNo ratings yet
- Biokimia Farmasi Asam Amino, Oligopeptida, Protein Serta Metabolisme Asam Amino Dan ProteinDocument52 pagesBiokimia Farmasi Asam Amino, Oligopeptida, Protein Serta Metabolisme Asam Amino Dan ProteinCHEISY ANASTASYA GRATIA LENGKONG100% (1)
- Drug Related ProblemDocument13 pagesDrug Related ProblemLinda Yuni LestariNo ratings yet
- 275 280 Drug Related Problems Antipsikotik Pada Pasien Skizofrenia PDFDocument6 pages275 280 Drug Related Problems Antipsikotik Pada Pasien Skizofrenia PDFtiarasrisudarsihNo ratings yet
- Org STP Harm CareDocument3 pagesOrg STP Harm CarelatemmaNo ratings yet
- History of Pharmacy in IndiaDocument7 pagesHistory of Pharmacy in IndiaJaja Jaelani75% (4)
- Guidelines For The Administration of Drugs Through Enteral Feeding Tubes AnonDocument24 pagesGuidelines For The Administration of Drugs Through Enteral Feeding Tubes AnonChen Boon TeyNo ratings yet
- Symptoms and Prevention of TuberculosisDocument2 pagesSymptoms and Prevention of Tuberculosisnisa rahma andinaNo ratings yet
- Drug Utilization Review (DUR)Document8 pagesDrug Utilization Review (DUR)Rinta MoonNo ratings yet
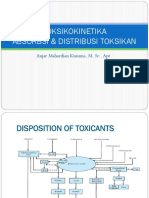
- Toksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptDocument51 pagesToksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptRossy OchieNo ratings yet
- TDM Dan Rancangan Aturan DosisDocument37 pagesTDM Dan Rancangan Aturan Dosisadelin ransunNo ratings yet
- Medicinus Agustus SmallDocument64 pagesMedicinus Agustus SmallNovry DodyNo ratings yet
- Drug InteractionDocument2 pagesDrug InteractionNicole EncinaresNo ratings yet
- AllopurinolDocument48 pagesAllopurinolFarha Elein KukihiNo ratings yet
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
- Ligand Efficiency Indices for Drug Discovery: Towards an Atlas-Guided ParadigmFrom EverandLigand Efficiency Indices for Drug Discovery: Towards an Atlas-Guided ParadigmNo ratings yet
- Pharmacogenomics: From Discovery to Clinical ImplementationFrom EverandPharmacogenomics: From Discovery to Clinical ImplementationShowkat Ahmad GanieNo ratings yet
- Estudio SEDCOMDocument11 pagesEstudio SEDCOMElias Vera RojasNo ratings yet
- Laporan Stoc ObatDocument34 pagesLaporan Stoc ObatAyouItuYustirahayuNo ratings yet
- Misoprostol Dosages For Reproductive HealthDocument1 pageMisoprostol Dosages For Reproductive HealthAnonymous b6xAErNo ratings yet
- Manufacturing Pharmaceuticals GuideDocument8 pagesManufacturing Pharmaceuticals GuideDaniel OmolewaNo ratings yet
- CCGP Handbook Oct 12 - CM2 PDFDocument21 pagesCCGP Handbook Oct 12 - CM2 PDFgod4alllNo ratings yet
- 1 Neuropathic Pain AlgorithmDocument2 pages1 Neuropathic Pain AlgorithmRazmin SicatNo ratings yet
- Drug AnalysisDocument3 pagesDrug Analysiskristel_nicole18yahoNo ratings yet
- Community PharmacyDocument26 pagesCommunity PharmacyAlpin Starr100% (1)
- Antibiotic Desensitization ProtocolsDocument7 pagesAntibiotic Desensitization ProtocolsMichael FreudigerNo ratings yet
- Tramadol HydrochlorideDocument157 pagesTramadol HydrochlorideShahid LatifNo ratings yet
- GOUT: A Guide to Diagnosis and TreatmentDocument14 pagesGOUT: A Guide to Diagnosis and TreatmentMichelle Chia JungNo ratings yet
- PEF Contract SummaryDocument10 pagesPEF Contract SummaryJimmyVielkindNo ratings yet
- Compounds and Chemicals ListDocument988 pagesCompounds and Chemicals ListEmerson Gomez0% (1)
- Controlled Drugs: Schedules List (Updated November 2015) : Schedule 1Document3 pagesControlled Drugs: Schedules List (Updated November 2015) : Schedule 1RonfermNo ratings yet
- Azithromycin Nursing ConsiderationsDocument2 pagesAzithromycin Nursing ConsiderationsKristine YoungNo ratings yet
- SO - APOTEK VIVA GENERIK DUKUH SETRO (21 May 2014)Document84 pagesSO - APOTEK VIVA GENERIK DUKUH SETRO (21 May 2014)Diditz Putera Bangsa100% (1)
- JurisprudenceDocument121 pagesJurisprudenceKate EvangelistaNo ratings yet
- Nigeria Medicine Prices PDFDocument71 pagesNigeria Medicine Prices PDFsumadhurainfoNo ratings yet
- Notice: Biological Products: Patent Extension Regulatory Review Period Determinations— Protamine Sulfate Injection, Etc.Document3 pagesNotice: Biological Products: Patent Extension Regulatory Review Period Determinations— Protamine Sulfate Injection, Etc.Justia.comNo ratings yet
- Aurobindo Pharma Receives USFDA Approval For Vancomycin Hydrochloride For Injection (Company Update)Document2 pagesAurobindo Pharma Receives USFDA Approval For Vancomycin Hydrochloride For Injection (Company Update)Shyam SunderNo ratings yet
- Adult Drug Calculations Formulae (To Be Given With Test)Document2 pagesAdult Drug Calculations Formulae (To Be Given With Test)DanielaNo ratings yet
- Renton T PDFDocument5 pagesRenton T PDFFelipe RoncerosNo ratings yet
- To Study The Effect of Hypnotics in Mice PDFDocument2 pagesTo Study The Effect of Hypnotics in Mice PDFSuman DahalNo ratings yet