You might also like
- Mandibulofacial Dysostosis, Also Known As Treacher CollinsDocument19 pagesMandibulofacial Dysostosis, Also Known As Treacher CollinsMoe KebabNo ratings yet
- Pediatric - Hearing - Loss Lau 3-17-10Document45 pagesPediatric - Hearing - Loss Lau 3-17-10Arief FakhrizalNo ratings yet
- Pedi HN SlidesDocument71 pagesPedi HN SlidesvelangniNo ratings yet
- CommonPedSyndromes PDFDocument89 pagesCommonPedSyndromes PDFdruzair007No ratings yet
- Legg Calve PerthesDocument93 pagesLegg Calve PerthesAkshay LakraNo ratings yet
- down syndrome.pdfDocument30 pagesdown syndrome.pdfAmany SaifNo ratings yet
- Múltiple Odontogenic Keratocysts: Presented By: Dr. Kush PathakDocument58 pagesMúltiple Odontogenic Keratocysts: Presented By: Dr. Kush PathakKush PathakNo ratings yet
- Pott’s Disease: A Concise OverviewDocument54 pagesPott’s Disease: A Concise OverviewDexter Flores100% (1)
- Congenital Malformations of The BrainDocument57 pagesCongenital Malformations of The Brainmanisha paikarayNo ratings yet
- DDHDocument174 pagesDDHVikas RaiNo ratings yet
- Craniofacial SyndromesDocument101 pagesCraniofacial SyndromesSaranya MohanNo ratings yet
- Annormalities of Fetal HeadDocument28 pagesAnnormalities of Fetal Headpathsala nursingNo ratings yet
- The Colobomaeye Syndrome - A Rare CasereportDocument11 pagesThe Colobomaeye Syndrome - A Rare CasereportIJAR JOURNALNo ratings yet
- Clinical Approach To The Dysmorphic Child-R-1Document108 pagesClinical Approach To The Dysmorphic Child-R-1Drbhupeshwari Gour100% (1)
- Cleodocranial Dysplasis 2018 Dr. KH ShivuteDocument22 pagesCleodocranial Dysplasis 2018 Dr. KH ShivuteKandiwapa ShivuteNo ratings yet
- Genetic Disorders: Chromosomal Abnormalities and Down SyndromeDocument27 pagesGenetic Disorders: Chromosomal Abnormalities and Down SyndromeMerwan KemalNo ratings yet
- Chromosomes: Structure of A ChromosomeDocument27 pagesChromosomes: Structure of A ChromosomeLaika LaiNo ratings yet
- Diseases and Treatment of CartilageDocument42 pagesDiseases and Treatment of Cartilageheena solankiNo ratings yet
- Clinical Diseases With Chromosomal AbnormalitiesDocument52 pagesClinical Diseases With Chromosomal AbnormalitiesAzifah ZakariaNo ratings yet
- Achondroplasia Guide: Causes, Symptoms & TreatmentDocument22 pagesAchondroplasia Guide: Causes, Symptoms & TreatmentA Nurfatiha JafarNo ratings yet
- CraniosynostosisDocument36 pagesCraniosynostosisFathima Jansi MalapatiNo ratings yet
- Pott'S Spine: Moderator: DR Peeyush SharmaDocument55 pagesPott'S Spine: Moderator: DR Peeyush SharmaRenie SerranoNo ratings yet
- Pott'S Spine: Moderator: DR Peeyush SharmaDocument55 pagesPott'S Spine: Moderator: DR Peeyush SharmaRenie SerranoNo ratings yet
- Treacher Collins Syndrome ExplainedDocument21 pagesTreacher Collins Syndrome ExplainedDIANA PAOLA FONTECHA GONZÁLEZNo ratings yet
- Treacher Collins SyndromeDocument21 pagesTreacher Collins SyndromeDIANA PAOLA FONTECHA GONZÁLEZNo ratings yet
- Cri Du ChatDocument16 pagesCri Du ChatJet LeeNo ratings yet
- Labioskisis Dan Palatoskisis: Pembimbing: Dr. Utama Abdi Tarigan, SP - Bp-Re (K)Document35 pagesLabioskisis Dan Palatoskisis: Pembimbing: Dr. Utama Abdi Tarigan, SP - Bp-Re (K)yenny purba0% (1)
- How To Describe Dysmorphic Features?: DR Bassam Y. Abu-Libdeh Makassed Hospital & Al-Quds Medical SchoolDocument43 pagesHow To Describe Dysmorphic Features?: DR Bassam Y. Abu-Libdeh Makassed Hospital & Al-Quds Medical SchoolMhmNo ratings yet
- Down Syndrome, Mental Retardation, Learning DisabilitiesDocument21 pagesDown Syndrome, Mental Retardation, Learning DisabilitiesMie CorsNo ratings yet
- OtosclerosisDocument36 pagesOtosclerosisShamsheer ShaikNo ratings yet
- Osteogenesis Imperfecta GuideDocument55 pagesOsteogenesis Imperfecta GuideNorman RiyadiNo ratings yet
- Otosclerosis & Acostic NeuromaDocument44 pagesOtosclerosis & Acostic NeuromaAbdullah AnsarNo ratings yet
- Lecture 6 Congenital Bone DisorderDocument100 pagesLecture 6 Congenital Bone DisorderWilson HalimNo ratings yet
- 0 Yazan Mini-OSCE PedsDocument60 pages0 Yazan Mini-OSCE Pedsmoyasserayoub78No ratings yet
- Long Face SyndromeDocument144 pagesLong Face Syndromeavanthika krishnaraj100% (2)
- Neurology ExaminationDocument31 pagesNeurology ExaminationEtana AdamNo ratings yet
- Cranial Nerves FunctionsDocument6 pagesCranial Nerves FunctionsAraceli Ecot CalunodNo ratings yet
- Treacher Collins Syndrome Comprehensi - 2004 - Oral and Maxillofacial Surgery CDocument21 pagesTreacher Collins Syndrome Comprehensi - 2004 - Oral and Maxillofacial Surgery Claljadeff12No ratings yet
- Transient Hip SynovitisDocument43 pagesTransient Hip SynovitisnurulNo ratings yet
- Pediatric Neurologic DisordersDocument97 pagesPediatric Neurologic DisordersMa Tosca Cybil TorresNo ratings yet
- Pediatric Brain Tumor Imaging CasesDocument81 pagesPediatric Brain Tumor Imaging CasesghassanNo ratings yet
- Anaesthetic Management Branchial Oto Renal SyndromeDocument5 pagesAnaesthetic Management Branchial Oto Renal SyndromeJIHAN ISMAILNo ratings yet
- Pediatric Endocrine Review - Part 5Document27 pagesPediatric Endocrine Review - Part 5Vicheth SenNo ratings yet
- MFD Part2 Pastpapers According To SubjectsDocument255 pagesMFD Part2 Pastpapers According To SubjectsEnea Nastri100% (3)
- TRUMADocument56 pagesTRUMAzainabd1964No ratings yet
- Down'S Syndrome: Also Known As MongolismDocument51 pagesDown'S Syndrome: Also Known As Mongolismlicurici_love_pacifiNo ratings yet
- Spinal Deformities (Congenital)Document27 pagesSpinal Deformities (Congenital)deathmetal017No ratings yet
- Fetal CaseDocument43 pagesFetal Casemomina zulfeenNo ratings yet
- ORAL SOFT TISSUE ABNORMALITIES: A REVIEWDocument123 pagesORAL SOFT TISSUE ABNORMALITIES: A REVIEWZulekha BegumNo ratings yet
- Neural Tube Defects (NTDS)Document59 pagesNeural Tube Defects (NTDS)Syed ShahNo ratings yet
- Metabolic Genetic DiseasesDocument77 pagesMetabolic Genetic DiseasesZNo ratings yet
- Neural Tube DefectDocument43 pagesNeural Tube DefectEllen AngelNo ratings yet
- DOC-20231126-WA0009.Document14 pagesDOC-20231126-WA0009.jalional20No ratings yet
- CherubismDocument12 pagesCherubismSureeratPatima100% (1)
- Perthes Disease: by Dr. Abdul Karim Postgraduate Resident Orthopedic Surgery Pgmi/Lgh. Lahore PakistanDocument68 pagesPerthes Disease: by Dr. Abdul Karim Postgraduate Resident Orthopedic Surgery Pgmi/Lgh. Lahore Pakistandrakkashmiri50% (2)
- Cerebral Palsy: MBBS YEAR 3, Batch 8, 2019 DR - Swe Zin Aye Zinaye - Swe@qiup - Edu.myDocument37 pagesCerebral Palsy: MBBS YEAR 3, Batch 8, 2019 DR - Swe Zin Aye Zinaye - Swe@qiup - Edu.myVishalli KalaiwananNo ratings yet
- CR Couzon SyndromeDocument3 pagesCR Couzon SyndromeDevi RistikaNo ratings yet
- RADIOLOGI - NEURORADIOLOGI 2 - Dr. Farah - Kelas ADocument106 pagesRADIOLOGI - NEURORADIOLOGI 2 - Dr. Farah - Kelas ASeno TanubrataNo ratings yet
- Jama Bates 2021 LD 210045 1626868722.2071Document2 pagesJama Bates 2021 LD 210045 1626868722.2071Moe KebabNo ratings yet
- Heart Failure Presentation Internal MedDocument1 pageHeart Failure Presentation Internal MedMoe KebabNo ratings yet
- Jama Diaz 2021 LD 210051 1627992112.38089Document3 pagesJama Diaz 2021 LD 210051 1627992112.38089Moe KebabNo ratings yet
- General Principles - AdditionsDocument3 pagesGeneral Principles - AdditionsMoe KebabNo ratings yet
- Antiamoebic DrugsDocument23 pagesAntiamoebic DrugsMoe KebabNo ratings yet
- BronchiolitisDocument29 pagesBronchiolitisMoe KebabNo ratings yet
- 2494d1335984469 Goljan RR Pathology Based Flashcards PDF Download Acid BaseDocument56 pages2494d1335984469 Goljan RR Pathology Based Flashcards PDF Download Acid BasejettyvikasNo ratings yet
- Biochemistry PDFDocument47 pagesBiochemistry PDFMoe KebabNo ratings yet
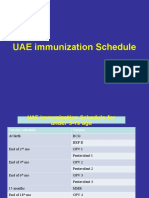
- Immunization Schedule UAEDocument3 pagesImmunization Schedule UAEMoe KebabNo ratings yet
- Psychotic Disorders MedhatDocument17 pagesPsychotic Disorders MedhatMoe Kebab100% (1)
- Goljan 5 Days (125 PGS)Document125 pagesGoljan 5 Days (125 PGS)heartofanmd95% (21)
- NystagmusDocument8 pagesNystagmusMoe KebabNo ratings yet
- Psychiatric EmergencyDocument33 pagesPsychiatric EmergencyMoe KebabNo ratings yet
- Tapeworms: Cestodes and Their Life CyclesDocument22 pagesTapeworms: Cestodes and Their Life CyclesMoe KebabNo ratings yet
- Acs ShortDocument13 pagesAcs ShortMoe KebabNo ratings yet
- 2015samples Step1Document45 pages2015samples Step1katherineNo ratings yet
- Obg Physical ExamDocument3 pagesObg Physical ExamMoe KebabNo ratings yet
- Neonatal Sepsis Signs, Risk Factors, and TreatmentDocument18 pagesNeonatal Sepsis Signs, Risk Factors, and TreatmentMoe KebabNo ratings yet
- Human Resource Management: Submitted By: Group # 6 Submitted To: Sir Usama NajamDocument23 pagesHuman Resource Management: Submitted By: Group # 6 Submitted To: Sir Usama NajamkamranNo ratings yet
- Effects of Sucrose Concentration On Cell Respiration in YeastDocument7 pagesEffects of Sucrose Concentration On Cell Respiration in YeastRachel Utomo83% (23)
- Year 8 Drama ScriptDocument8 pagesYear 8 Drama ScriptTISMSecondaryNo ratings yet
- KPI and Supplier Performance Scorecard ToolDocument7 pagesKPI and Supplier Performance Scorecard ToolJayant Kumar JhaNo ratings yet
- Measles/ Rubella & VPD Surveillance:: Allotment of EPID Number and Outbreak IDDocument7 pagesMeasles/ Rubella & VPD Surveillance:: Allotment of EPID Number and Outbreak IDDevendra Singh TomarNo ratings yet
- Materi Bahasa Inggris Kelas 9 - LabelsDocument12 pagesMateri Bahasa Inggris Kelas 9 - LabelsEnglish Is fun67% (3)
- Chemistry Tshirt ProjectDocument7 pagesChemistry Tshirt Projectapi-524483093No ratings yet
- Self-Adhesive Resin Cements Ph-Neutralization, HydrophilicityDocument7 pagesSelf-Adhesive Resin Cements Ph-Neutralization, HydrophilicityCarolina Rodríguez RamírezNo ratings yet
- Companies Directory Alternative Fuels and Smart Transportation June 20Document82 pagesCompanies Directory Alternative Fuels and Smart Transportation June 20Mbamali Chukwunenye100% (1)
- Civil-Engineering-Final-Year-Project-Quarry Dust As A Substitute of River Sand in Concrete Mixes PDFDocument75 pagesCivil-Engineering-Final-Year-Project-Quarry Dust As A Substitute of River Sand in Concrete Mixes PDFVEERKUMAR GNDEC100% (1)
- Book 1Document100 pagesBook 1Devasyruc100% (1)
- History of Medicine - Alexander WilderDocument555 pagesHistory of Medicine - Alexander WilderMark R. JaquaNo ratings yet
- Food ProcessingDocument5 pagesFood ProcessingMarycris Doria100% (2)
- Annotated Bibliography Graphic OrganizerDocument4 pagesAnnotated Bibliography Graphic Organizerapi-348035481No ratings yet
- Certificate of Employment Document TitleDocument1 pageCertificate of Employment Document TitleAyni ReyesNo ratings yet
- Weld Procedure Specification (WPS) : Joint Design Welding SequenceDocument1 pageWeld Procedure Specification (WPS) : Joint Design Welding SequenceRicardo SoaresNo ratings yet
- Yoga Nidra MethodDocument13 pagesYoga Nidra MethodPrahlad Basnet100% (2)
- Assessments and Rubrics For Unit 2Document13 pagesAssessments and Rubrics For Unit 2api-302258576No ratings yet
- Escala de Violencia e Índice de SeveridadDocument11 pagesEscala de Violencia e Índice de SeveridadpsiserviciosprofesioNo ratings yet
- Bioreactor For Air Pollution ControlDocument6 pagesBioreactor For Air Pollution Controlscarmathor90No ratings yet
- Manual Murray 20Document28 pagesManual Murray 20freebanker777741No ratings yet
- Cobb 500 PDFDocument14 pagesCobb 500 PDFNeil Ryan100% (1)
- SinogramDocument2 pagesSinogramNguyễn Thành CôngNo ratings yet
- Rorschach y SuicidioDocument17 pagesRorschach y SuicidioLaura SierraNo ratings yet
- GP Series Portable Generator: Owner's ManualDocument48 pagesGP Series Portable Generator: Owner's ManualWilliam Medina CondorNo ratings yet
- Rexnord Thomas Flexible Disc Couplings - Series 71 - 8Document2 pagesRexnord Thomas Flexible Disc Couplings - Series 71 - 8Orlando ReisNo ratings yet
- 2013 - Sara E. TraceDocument35 pages2013 - Sara E. TraceDewi WulandariNo ratings yet
- Prosecution and elements of crimes under Philippine lawsDocument14 pagesProsecution and elements of crimes under Philippine lawsNoel Cagigas FelongcoNo ratings yet
- Extraction and Isolation of Saponins PDFDocument2 pagesExtraction and Isolation of Saponins PDFMikeNo ratings yet
- Save and share GZCL training spreadsheets onlineDocument263 pagesSave and share GZCL training spreadsheets onlinejohn wick100% (1)