You might also like
- Epidemiology: Disease in The U.S. Pathogenesis Clinical Manifestations Diagnosis Patient Management PreventionDocument52 pagesEpidemiology: Disease in The U.S. Pathogenesis Clinical Manifestations Diagnosis Patient Management PreventionxohanortNo ratings yet
- Gonorrhea: Neisseria GonorrhoeaeDocument60 pagesGonorrhea: Neisseria GonorrhoeaeRikki OkNo ratings yet
- Chlamydia SlidesDocument63 pagesChlamydia SlidesEspecialistaLanderNo ratings yet
- Vaginitis: - Trichomoniasis - Vulvovaginal Candidiasis (VVC) - Bacterial Vaginosis (BV)Document94 pagesVaginitis: - Trichomoniasis - Vulvovaginal Candidiasis (VVC) - Bacterial Vaginosis (BV)Munkhjargal BatmunkhNo ratings yet
- Pelvic Inflammatory Disease (PID)Document43 pagesPelvic Inflammatory Disease (PID)Asghar AliNo ratings yet
- Gonorrhea-Slides 2020Document47 pagesGonorrhea-Slides 2020El-rohyKalongoNo ratings yet
- Quizz 1 Review Advanced IIDocument66 pagesQuizz 1 Review Advanced IIamelyNo ratings yet
- Pelvic Inflammatory DiseaseDocument41 pagesPelvic Inflammatory DiseaseEvellyna MeilanyNo ratings yet
- PID LectureDocument41 pagesPID LectureHarold Gabriel Sanchez DelgadoNo ratings yet
- GYN 讀書報告Document67 pagesGYN 讀書報告Chia-Yuan ChenNo ratings yet
- STIs O & GDocument59 pagesSTIs O & GNoraNo ratings yet
- CDC 4 STDDocument67 pagesCDC 4 STDdemessie diribaNo ratings yet
- Pelvic Inflammatory DiseaseDocument10 pagesPelvic Inflammatory DiseaseMuhammad IqbalNo ratings yet
- Sexually Transmitted Diseases : (Gonorrhea, Syphilis & Aids)Document54 pagesSexually Transmitted Diseases : (Gonorrhea, Syphilis & Aids)joel david knda mjNo ratings yet
- BMJ 335 7630 CR 01147 Vaginal DischargeDocument5 pagesBMJ 335 7630 CR 01147 Vaginal DischargeHassan Abdullah AL-balushiNo ratings yet
- Syphilis SlidesDocument85 pagesSyphilis SlidesSamuel Sebastian Sirapanji100% (1)
- Pneumonia in ChildrenDocument110 pagesPneumonia in ChildrenHabibullah AlNo ratings yet
- Pelvic Inflammatory DiseaseDocument8 pagesPelvic Inflammatory DiseaseKhairunNisaNo ratings yet
- Pelvic Inflammatory Disease: CDC 24/7: Saving Lives. Protecting PeopleDocument9 pagesPelvic Inflammatory Disease: CDC 24/7: Saving Lives. Protecting PeopleAmanda GANo ratings yet
- Guide to Pediatric Urology and Surgery in Clinical PracticeFrom EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNo ratings yet
- Sexually Transmitted InfectionDocument107 pagesSexually Transmitted Infectionanfalalamin9915No ratings yet
- Group: StudyDocument10 pagesGroup: StudyJovert Andrei DavidNo ratings yet
- STD OutlineDocument16 pagesSTD OutlineLory TangpusNo ratings yet
- Sexually Transmitted Infections: By-Nimco A. MDDocument89 pagesSexually Transmitted Infections: By-Nimco A. MDgibreilNo ratings yet
- BiologyDocument4 pagesBiologyJoane Rivera BontiaNo ratings yet
- Case 6 For TutorDocument9 pagesCase 6 For TutorwijiantotepasNo ratings yet
- Sexually Transmitted Infections-5Document5 pagesSexually Transmitted Infections-5diko_nalNo ratings yet
- Sexually Transmitted InfectionDocument24 pagesSexually Transmitted InfectionAnas Abdel Rihem0% (1)
- Gyne - (Section B) PID-STI-1Document45 pagesGyne - (Section B) PID-STI-1Kailash KhatriNo ratings yet
- WCLF E1 J 66 F YPUTf 0149Document165 pagesWCLF E1 J 66 F YPUTf 0149ClintonNo ratings yet
- UTIJournal PresentDocument21 pagesUTIJournal Presentsahsweta67No ratings yet
- Jurnal Acne 1Document12 pagesJurnal Acne 1riena456No ratings yet
- Pelvic Inflammatory DiseaseDocument25 pagesPelvic Inflammatory DiseasedeepaNo ratings yet
- 公衛政策的基礎 流行病學nDocument70 pages公衛政策的基礎 流行病學nKkggvvNo ratings yet
- Vaginal Discharge: Clinical ReviewDocument5 pagesVaginal Discharge: Clinical ReviewOktari Dwi YantiNo ratings yet
- Gynecology Case Formulation Group-2 Section-BDocument25 pagesGynecology Case Formulation Group-2 Section-Bastak ghisingNo ratings yet
- By: Jennifer Vu, Teresa Kodi, Emily Dang, James Baawuo and Yesenia AlmanzaDocument19 pagesBy: Jennifer Vu, Teresa Kodi, Emily Dang, James Baawuo and Yesenia AlmanzajbaawuoNo ratings yet
- Sexually Transmitted DiseasesDocument71 pagesSexually Transmitted DiseasesAkwu AkwuNo ratings yet
- Introduction To Epidemiology Presented by L. MuparaDocument107 pagesIntroduction To Epidemiology Presented by L. MuparaArwen WellingtonNo ratings yet
- Reproductive Tract InfectionDocument48 pagesReproductive Tract InfectionSampriti Roy100% (1)
- Chlamydia and Nonspecific UrethritisDocument4 pagesChlamydia and Nonspecific UrethritisErfina BasriNo ratings yet
- 2 PidDocument31 pages2 PidNatif BoteNo ratings yet
- RTI/STI Prevalence in Selected Sites in The Philippines: Department of HealthDocument68 pagesRTI/STI Prevalence in Selected Sites in The Philippines: Department of HealthMaricel SalinasNo ratings yet
- StdsDocument71 pagesStdsabel semuNo ratings yet
- Prevalence of Urinary Tract Infections and Their Antibiotic Sensitivity in Tertiary Care Hospital LahoreDocument5 pagesPrevalence of Urinary Tract Infections and Their Antibiotic Sensitivity in Tertiary Care Hospital LahoreInternational Organization of Scientific Research (IOSR)No ratings yet
- Orchits ManagementDocument9 pagesOrchits ManagementMarshall ThompsonNo ratings yet
- National Health Programs in Nepal: Prof. Dr. I.DudaniDocument89 pagesNational Health Programs in Nepal: Prof. Dr. I.DudaniboomboompakNo ratings yet
- Reproductive Tract InformationDocument14 pagesReproductive Tract InformationGonçalo BaptistaNo ratings yet
- STi PresentationDocument20 pagesSTi PresentationPheywood1234No ratings yet
- Uti PediaDocument8 pagesUti PediaNeenya SisonNo ratings yet
- Introduction To Epidemiology: The Basic Science of Public HealthDocument34 pagesIntroduction To Epidemiology: The Basic Science of Public Healthapi-19641337100% (1)
- STI HIV, PMTCT, Abnormal Vagina L Discharge and Genital Ulcers EditedDocument60 pagesSTI HIV, PMTCT, Abnormal Vagina L Discharge and Genital Ulcers Editedsirgute tamratNo ratings yet
- Gonorrhoea 2006Document8 pagesGonorrhoea 2006Sanveer AthwalNo ratings yet
- Case Study GonorrheaDocument19 pagesCase Study GonorrheaErika ThereseNo ratings yet
- Diagnosis of Urinary Tract Infections in ChildrenDocument31 pagesDiagnosis of Urinary Tract Infections in ChildrennurmawinawanNo ratings yet
- Sexually Transmitted Diseases - Part 1: DR Clarissa ListerDocument20 pagesSexually Transmitted Diseases - Part 1: DR Clarissa Listerandreas kevinNo ratings yet
- Hum. Reprod.-2013-Romosan-1569-79Document11 pagesHum. Reprod.-2013-Romosan-1569-79Ahmad Arbi AninditoNo ratings yet
- Sexually Transmitted Diseases: Isaac F. Mitropoulos, Pharm.DDocument8 pagesSexually Transmitted Diseases: Isaac F. Mitropoulos, Pharm.Djculllum100% (1)
- DDD DDDD DDDD DDDDDocument1 pageDDD DDDD DDDD DDDDYonathanHasudunganNo ratings yet
- G GGGGG GGGGG GGGGG GGGGGDocument1 pageG GGGGG GGGGG GGGGG GGGGGYonathanHasudunganNo ratings yet
- E Eeeeeeeeeeeeeee EeeeeeeeeeeeeeeDocument1 pageE Eeeeeeeeeeeeeee EeeeeeeeeeeeeeeYonathanHasudunganNo ratings yet
- AaaaaaaaaaaaaaaaaaaaaaDocument1 pageAaaaaaaaaaaaaaaaaaaaaaYonathanHasudunganNo ratings yet
- I Iiiiii IiiiiiDocument1 pageI Iiiiii IiiiiiYonathanHasudunganNo ratings yet
- LL LLLLL LLLLL LLLLLDocument1 pageLL LLLLL LLLLL LLLLLYonathanHasudunganNo ratings yet
- AaaaaaaaaaaaaaaaaaaaaaDocument1 pageAaaaaaaaaaaaaaaaaaaaaaYonathanHasudunganNo ratings yet
- EeeeeeeeeeeeeeeeDocument1 pageEeeeeeeeeeeeeeeeYonathanHasudunganNo ratings yet
- AaaaaaaaaaaaaaaDocument1 pageAaaaaaaaaaaaaaaYonathanHasudunganNo ratings yet
- AaaaaaaaaaaaaaaDocument1 pageAaaaaaaaaaaaaaaYonathanHasudunganNo ratings yet
- DDD DDDD DDDD DDDDDocument1 pageDDD DDDD DDDD DDDDYonathanHasudunganNo ratings yet
- E EeeeeeeeeeeeeeeDocument1 pageE EeeeeeeeeeeeeeeYonathanHasudunganNo ratings yet
- DengueDocument38 pagesDenguevoruganty_vvsNo ratings yet
- AaaaaaaaaaaaaaaDocument1 pageAaaaaaaaaaaaaaaYonathanHasudunganNo ratings yet
- A AaaaaaaaaaaaDocument1 pageA AaaaaaaaaaaaYonathanHasudunganNo ratings yet
- DDDD DDDD DDDDDocument1 pageDDDD DDDD DDDDYonathanHasudunganNo ratings yet
- A AaaaaaaaaaaaaaaDocument1 pageA AaaaaaaaaaaaaaaYonathanHasudunganNo ratings yet
- GGGG GGGGG GGGGG GGGGGDocument1 pageGGGG GGGGG GGGGG GGGGGYonathanHasudunganNo ratings yet
- Eeeeeeeeeeee EeeeeeeeeeeeDocument1 pageEeeeeeeeeeee EeeeeeeeeeeeYonathanHasudunganNo ratings yet
- DDD DDDD DDDDDocument1 pageDDD DDDD DDDDYonathanHasudunganNo ratings yet
- A A A A AaaaaaaaaaaaaaaDocument1 pageA A A A AaaaaaaaaaaaaaaYonathanHasudunganNo ratings yet
- A A A A AaaaaaaaaaaaaaaDocument1 pageA A A A AaaaaaaaaaaaaaaYonathanHasudunganNo ratings yet
- Calling Visa MenteriDocument1 pageCalling Visa MenteriYonathanHasudunganNo ratings yet
- Visscher GonorrheaDocument58 pagesVisscher GonorrheacenmeriNo ratings yet
- Typhoid Fever Interna NewDocument41 pagesTyphoid Fever Interna NewSisilia AlfinaNo ratings yet
- COVER Ujian Status MataDocument1 pageCOVER Ujian Status MataYonathanHasudunganNo ratings yet
- Typhoid Fever Interna NewDocument41 pagesTyphoid Fever Interna NewSisilia AlfinaNo ratings yet
- Typhoid Fever Interna NewDocument41 pagesTyphoid Fever Interna NewSisilia AlfinaNo ratings yet
- Pankreatitis IpdDocument28 pagesPankreatitis IpdYonathanHasudunganNo ratings yet
- Standard Treatment ProtocolsDocument663 pagesStandard Treatment Protocolsdrvins1No ratings yet
- 2021 Abbott Annual ReportDocument86 pages2021 Abbott Annual ReportAdriano BolgenhagenNo ratings yet
- ECPM 2021 European Congress of Perinatal MedicineDocument1 pageECPM 2021 European Congress of Perinatal MedicineAl DiNo ratings yet
- Fixed FunctionalDocument14 pagesFixed FunctionalsuchitraNo ratings yet
- 2005 PDFDocument436 pages2005 PDFAbdulazizNo ratings yet
- Ncp-Proper Sonia FinalDocument4 pagesNcp-Proper Sonia FinalSoniaMarieBalanayNo ratings yet
- MCC SaeDocument98 pagesMCC SaeAllison100% (1)
- Fcimb 12 962470Document15 pagesFcimb 12 962470wiwiNo ratings yet
- Odb CdiDocument644 pagesOdb CdiPaul JagdharryNo ratings yet
- Peds EORDocument29 pagesPeds EORAndrew BowmanNo ratings yet
- UGRD-PECTM6358 Medical and Wellness TourismDocument12 pagesUGRD-PECTM6358 Medical and Wellness TourismRonalyn C. CariasNo ratings yet
- Rcse9702 115 s1Document1 pageRcse9702 115 s1WayyuNo ratings yet
- Task 17: Dosen PembmbingDocument3 pagesTask 17: Dosen PembmbingRif'an KhaliliNo ratings yet
- Anees, Prijecth SjebevwhDocument3 pagesAnees, Prijecth SjebevwhAkNo ratings yet
- Nursing Informatics-Innovative Technology in HealthDocument2 pagesNursing Informatics-Innovative Technology in HealthAnonymous izrFWiQ100% (1)
- Infection Control Practice On Vital Signs Equipment: A Survey Among Senior Nursing Students in Iloilo City, PhilippinesDocument7 pagesInfection Control Practice On Vital Signs Equipment: A Survey Among Senior Nursing Students in Iloilo City, PhilippinesRyan Michael OducadoNo ratings yet
- s9 Basic Life SupportDocument27 pagess9 Basic Life SupportputuNo ratings yet
- Final Pre Accreditation Entry Level Standards For Hospital Book PDFDocument53 pagesFinal Pre Accreditation Entry Level Standards For Hospital Book PDFams_1234100% (1)
- The Caregiver Training CurriculumDocument10 pagesThe Caregiver Training CurriculumOlaya alghareniNo ratings yet
- Hypertensive Emergency 3Document45 pagesHypertensive Emergency 3saldy meirisandyNo ratings yet
- Mmha EcoDocument54 pagesMmha EcoAlfredo De Ocampo JrNo ratings yet
- Astaxanthin Uses and Effectiveness in Therapy of Acnes Vulgaris Final Revisi 7Document12 pagesAstaxanthin Uses and Effectiveness in Therapy of Acnes Vulgaris Final Revisi 7Desica NatalisaNo ratings yet
- Pakistan Hand Hygiene For All Roadmap DocumentDocument30 pagesPakistan Hand Hygiene For All Roadmap DocumentNiazullah KhanNo ratings yet
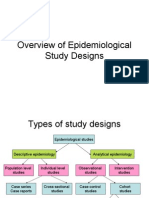
- Overview of Epidemiological Study DesignsDocument16 pagesOverview of Epidemiological Study DesignsLakshmi Seth100% (2)
- Model Kemitraan Puskesmas-Praktisi Swasta Dalam Penanggulangan Tuberkulosis Paru Di Kecamatan Kalasan, Kabupaten Sleman, Provinsi DiyDocument9 pagesModel Kemitraan Puskesmas-Praktisi Swasta Dalam Penanggulangan Tuberkulosis Paru Di Kecamatan Kalasan, Kabupaten Sleman, Provinsi DiyDesvolim DesoNo ratings yet
- Orthostatic Hypotension (Postural Hypotension) - Symptoms and Causes - Mayo ClinicDocument1 pageOrthostatic Hypotension (Postural Hypotension) - Symptoms and Causes - Mayo Clinicruba al hammadiNo ratings yet
- Ventilator Associated Pneumonia and GuidelinesDocument28 pagesVentilator Associated Pneumonia and GuidelineshawinnurdianaNo ratings yet
- Ambulatory Care Medical Surgical NursingDocument11 pagesAmbulatory Care Medical Surgical NursingNiña Antoniette Gutang100% (4)
- Ethics Essential For Usmle Step 1 ExamDocument48 pagesEthics Essential For Usmle Step 1 ExamJunaid AnwarNo ratings yet
- Global School-Based Student Health Survey: BackgroundDocument2 pagesGlobal School-Based Student Health Survey: BackgroundU Bagja PutraNo ratings yet