You might also like
- Addendum For PWBD For Online RegDocument1 pageAddendum For PWBD For Online Regprashanth100% (1)
- Notice Result Extend - NursingOfficer - 2019Document1 pageNotice Result Extend - NursingOfficer - 2019prashanthNo ratings yet
- Advt of Nursing Officer For 4 AIIMS - 1Document10 pagesAdvt of Nursing Officer For 4 AIIMS - 1prashanthNo ratings yet
- United India Insurance Recruitment for 300+ VacanciesDocument29 pagesUnited India Insurance Recruitment for 300+ VacanciesRavi SrivastavaNo ratings yet
- M.O.S.C.College of Nursing, Kolenchery 3Rd Year B.Sc. Nursing Degree Course (2013-17 Batch) Clinical PlanDocument12 pagesM.O.S.C.College of Nursing, Kolenchery 3Rd Year B.Sc. Nursing Degree Course (2013-17 Batch) Clinical PlanprashanthNo ratings yet
- Final Result - Nursing Officer Central Hospitals-2019-NETDocument17 pagesFinal Result - Nursing Officer Central Hospitals-2019-NETprashanthNo ratings yet
- Medical MalpracticeDocument41 pagesMedical MalpracticeprashanthNo ratings yet
- Project ReportDocument2 pagesProject ReportprashanthNo ratings yet
- Cghs Nabh Application HospitalDocument27 pagesCghs Nabh Application HospitalGaurav SharmaNo ratings yet
- HMIS Kerala RevisedDocument34 pagesHMIS Kerala RevisedprashanthNo ratings yet
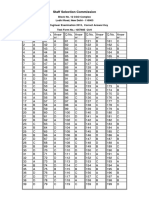
- SSC JE 2015 Exam Correct Answer Key for Test Form 1057685Document2 pagesSSC JE 2015 Exam Correct Answer Key for Test Form 1057685prashanthNo ratings yet
- Your Bibliography VancouverDocument1 pageYour Bibliography VancouverprashanthNo ratings yet
- OremDocument12 pagesOremprashanthNo ratings yet
- 8TIME TABLE - 2013 Batch Third YearDocument2 pages8TIME TABLE - 2013 Batch Third YearprashanthNo ratings yet
- Post Basic BSC Admn PlanDocument2 pagesPost Basic BSC Admn PlanprashanthNo ratings yet
- M.O.S.C College of Nursing Kolenchery: Anecdotal RecordDocument5 pagesM.O.S.C College of Nursing Kolenchery: Anecdotal RecordprashanthNo ratings yet
- 2TIME TABLE - 2013 Batch Third YearDocument2 pages2TIME TABLE - 2013 Batch Third YearprashanthNo ratings yet
- 2TIME TABLE - 2013 Batch Third YearDocument2 pages2TIME TABLE - 2013 Batch Third YearprashanthNo ratings yet
- Bowel IncontinenceDocument4 pagesBowel IncontinenceprashanthNo ratings yet
- Martha RogerDocument10 pagesMartha RogerprashanthNo ratings yet
- Physical ExaminationDocument39 pagesPhysical ExaminationprashanthNo ratings yet
- M.O.S.C.College of Nursing 3 Year BSC Nursing Pattern of ExaminationDocument1 pageM.O.S.C.College of Nursing 3 Year BSC Nursing Pattern of ExaminationprashanthNo ratings yet
- Seminar On BUDGETDocument14 pagesSeminar On BUDGETprashanth60% (5)
- ANP Clinical Rotation 2015 SinuDocument4 pagesANP Clinical Rotation 2015 SinuprashanthNo ratings yet
- Diabetic Foot Care OverviewDocument21 pagesDiabetic Foot Care Overviewprashanth100% (4)
- Unit Plan Mental Health NursingDocument2 pagesUnit Plan Mental Health Nursingprashanth100% (2)
- Calculation of Clinical HoursDocument1 pageCalculation of Clinical HoursprashanthNo ratings yet
- Assessment Format Mental Health NursingDocument11 pagesAssessment Format Mental Health Nursingprashanth100% (1)
- M.O.S.C College Psychiatric Nursing FormsDocument5 pagesM.O.S.C College Psychiatric Nursing FormsprashanthNo ratings yet
- Tuners SndromeDocument9 pagesTuners SndromeprashanthNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Tips For Establish Ball Pen Refill PlantDocument5 pagesTips For Establish Ball Pen Refill PlantSingam Sridhar100% (1)
- Mindray UMEC 12 Specifications FDADocument11 pagesMindray UMEC 12 Specifications FDAAlejandra Baas GuzmánNo ratings yet
- DSI-DYWIDAG Geotechnics Rock Bolts enDocument6 pagesDSI-DYWIDAG Geotechnics Rock Bolts enTomás Nunes da SilvaNo ratings yet
- PKL Geri RevDocument3 pagesPKL Geri RevKurniati NiaNo ratings yet
- ABO BLOOD GROUP Part 1Document104 pagesABO BLOOD GROUP Part 1Taladua Cayla Grace O.No ratings yet
- O-Rings & SealsDocument10 pagesO-Rings & SealsPartsGopher.comNo ratings yet
- Best WiFi Adapter For Kali Linux - Monitor Mode & Packet InjectionDocument14 pagesBest WiFi Adapter For Kali Linux - Monitor Mode & Packet InjectionKoushikNo ratings yet
- Paper TropicsDocument8 pagesPaper Tropicsdarobin21No ratings yet
- Pnp-MemorandumDocument9 pagesPnp-MemorandumraalphNo ratings yet
- 2.9&10 Synthesis Adn Stereoisomerism Exam Qs - 4Document4 pages2.9&10 Synthesis Adn Stereoisomerism Exam Qs - 4sureshthevanNo ratings yet
- Evonik Copi BrochureDocument5 pagesEvonik Copi BrochureRovshan HasanzadeNo ratings yet
- SKC EPAM-5000 Instruction Manual PDFDocument90 pagesSKC EPAM-5000 Instruction Manual PDFmegacobNo ratings yet
- Tennessee Medicaid Claimed Hundreds of Millions of Federal Funds For Certified Public Expenditures That Were Not in Compliance With Federal RequirementsDocument36 pagesTennessee Medicaid Claimed Hundreds of Millions of Federal Funds For Certified Public Expenditures That Were Not in Compliance With Federal RequirementsFOX 17 NewsNo ratings yet
- Butterfly Valve ConcentricDocument6 pagesButterfly Valve ConcentricpramodtryNo ratings yet
- QCVN 162019BXD National Technical Regulation On Products, Goods of Building Materials (Eng)Document41 pagesQCVN 162019BXD National Technical Regulation On Products, Goods of Building Materials (Eng)lwin_oo2435No ratings yet
- Glaus Corp. inventory note amortization adjusting entryDocument5 pagesGlaus Corp. inventory note amortization adjusting entryPatrick HarponNo ratings yet
- Quickscan™ Lite Qw2100: Multi-Purpose Uses For Different ApplicationsDocument2 pagesQuickscan™ Lite Qw2100: Multi-Purpose Uses For Different ApplicationsHaythem BchirNo ratings yet
- The Magnetic GazeDocument126 pagesThe Magnetic GazeTomico TTNo ratings yet
- Original Instruction Manual: Hypro Series 9303Document24 pagesOriginal Instruction Manual: Hypro Series 9303vandoNo ratings yet
- NCPDocument18 pagesNCPChristian Karl B. LlanesNo ratings yet
- Save Our Forests Through Sustainable DevelopmentDocument33 pagesSave Our Forests Through Sustainable DevelopmentGeehthanJINo ratings yet
- Fem 3202-1 IntroductionDocument29 pagesFem 3202-1 IntroductionRon ChongNo ratings yet
- TVL ICT IllustrationNCII Q1Module2Document12 pagesTVL ICT IllustrationNCII Q1Module2Kimberly Trocio Kim100% (1)
- Calcul BADocument15 pagesCalcul BAHanane BenGamraNo ratings yet
- Stakeholders in The Iep Process JDocument9 pagesStakeholders in The Iep Process Japi-546526887No ratings yet
- Corrosion and Its Objective QuestionsDocument2 pagesCorrosion and Its Objective QuestionsSrinivasan Alagappan100% (4)
- Data SheetDocument15 pagesData SheetLucian Sorin BortosuNo ratings yet
- Final Draft - Banana ChipsDocument34 pagesFinal Draft - Banana ChipsAubrey Delgado74% (35)
- Inspection and Repair of Aircraft Integral Tanks AND Fuel CellsDocument222 pagesInspection and Repair of Aircraft Integral Tanks AND Fuel CellsgnanasekarNo ratings yet
- PerforationsDocument5 pagesPerforationsMariusNONo ratings yet