You might also like
- Surface Emg For Back... ValidtyDocument2 pagesSurface Emg For Back... ValidtyMihir_Mehta_5497No ratings yet
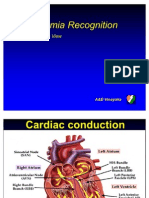
- Arrythmia RecognitionDocument79 pagesArrythmia RecognitionMihir_Mehta_5497100% (2)
- Examination of The Cardiovascular SystemDocument2 pagesExamination of The Cardiovascular Systemkenners98% (44)
- Ecg InterpritestionDocument35 pagesEcg InterpritestionMihir_Mehta_5497100% (1)
- Physio Therapy Modalities in R.A (Rhematoid Arthritis)Document9 pagesPhysio Therapy Modalities in R.A (Rhematoid Arthritis)Mihir_Mehta_5497No ratings yet
- Role of Physiotherapy in RaDocument60 pagesRole of Physiotherapy in RaMihir_Mehta_5497No ratings yet
- Maternal Health: Ekta Modi 2 MPT in RehabDocument368 pagesMaternal Health: Ekta Modi 2 MPT in RehabMihir_Mehta_5497100% (1)
- Joint MobilizationDocument23 pagesJoint MobilizationMihir_Mehta_549750% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cavitation in Francis PDFDocument373 pagesCavitation in Francis PDFAlberto AliagaNo ratings yet
- Grammar and Oral Language Development (GOLD) : Reported By: Melyn A. Bacolcol Kate Batac Julie Ann OcampoDocument17 pagesGrammar and Oral Language Development (GOLD) : Reported By: Melyn A. Bacolcol Kate Batac Julie Ann Ocampoclara dupitasNo ratings yet
- Module No.3 Prepare Architectual Job Requirements Architectural Working DrawingDocument23 pagesModule No.3 Prepare Architectual Job Requirements Architectural Working DrawingJay S. On100% (1)
- 面向2035的新材料强国战略研究 谢曼Document9 pages面向2035的新材料强国战略研究 谢曼hexuan wangNo ratings yet
- MKT STGDocument106 pagesMKT STGAmeya Singh RajputNo ratings yet
- 1and5.microscopes, Specializedstem Cells, Homeostasis - Answer KeyDocument1 page1and5.microscopes, Specializedstem Cells, Homeostasis - Answer KeyMCarmen López CastroNo ratings yet
- Fashion Goes VirtualDocument1 pageFashion Goes VirtualJessica MichaultNo ratings yet
- New Python Basics AssignmentDocument5 pagesNew Python Basics AssignmentRAHUL SONI0% (1)
- Software Requirements SpecificationDocument9 pagesSoftware Requirements SpecificationSu-kEm Tech LabNo ratings yet
- Painting: 22.1 Types of PaintsDocument8 pagesPainting: 22.1 Types of PaintsRosy RoseNo ratings yet
- Course Specifications: Fire Investigation and Failure Analysis (E901313)Document2 pagesCourse Specifications: Fire Investigation and Failure Analysis (E901313)danateoNo ratings yet
- Unknown 31Document40 pagesUnknown 31Tina TinaNo ratings yet
- Consumer Price SummaryDocument5 pagesConsumer Price SummaryKJ HiramotoNo ratings yet
- My Report in Assessment 1Document67 pagesMy Report in Assessment 1Eddie Wilson BroquezaNo ratings yet
- Syllabus Math 305Document4 pagesSyllabus Math 305Nataly SusanaNo ratings yet
- Preprints201808 0216 v1Document15 pagesPreprints201808 0216 v1Baptista Jaime MilioneNo ratings yet
- Almutairy / Musa MR: Boarding PassDocument1 pageAlmutairy / Musa MR: Boarding PassMusaNo ratings yet
- A Modified Linear Programming Method For Distribution System ReconfigurationDocument6 pagesA Modified Linear Programming Method For Distribution System Reconfigurationapi-3697505No ratings yet
- Bangalore Escorts Services - Riya ShettyDocument11 pagesBangalore Escorts Services - Riya ShettyRiya ShettyNo ratings yet
- MCQs + SEQs Medical Physics Midterm Exam Paper-Fall 2020Document3 pagesMCQs + SEQs Medical Physics Midterm Exam Paper-Fall 2020Ali Nouman100% (1)
- Far 2 Quiz 03212024Document6 pagesFar 2 Quiz 03212024red118831No ratings yet
- Aui2601 Exam Pack 2016 1Document57 pagesAui2601 Exam Pack 2016 1ricara alexia moodleyNo ratings yet
- 20171025141013chapter-3 Chi-Square-Test PDFDocument28 pages20171025141013chapter-3 Chi-Square-Test PDFNajwa WawaNo ratings yet
- BCSS Sec Unit 1 Listening and Speaking SkillsDocument16 pagesBCSS Sec Unit 1 Listening and Speaking Skillsjiny benNo ratings yet
- FixDocument4 pagesFixReza FahmiNo ratings yet
- 04 10 ALINT DatasheetDocument2 pages04 10 ALINT DatasheetJoakim LangletNo ratings yet
- Alpha Tech India Limited - FinalDocument4 pagesAlpha Tech India Limited - FinalRahul rNo ratings yet
- Yusuf Mahmood CVDocument3 pagesYusuf Mahmood CVapi-527941238No ratings yet
- AXIOM75 50 25 1B - Rev.6 10.000MHzDocument4 pagesAXIOM75 50 25 1B - Rev.6 10.000MHzTürkay PektürkNo ratings yet
- Toeic VocabularyDocument10 pagesToeic VocabularyBrian Niblo80% (5)