You might also like
- Anatomy L: Wajiha Nawabi MDDocument127 pagesAnatomy L: Wajiha Nawabi MDabdul wahabNo ratings yet
- Skeletal System: IB Sport, Exercise and Health ScienceDocument33 pagesSkeletal System: IB Sport, Exercise and Health ScienceMaggie-Louise BellamyNo ratings yet
- Introduction To The Study of Anatomy: BY Roel Cobarde M.DDocument55 pagesIntroduction To The Study of Anatomy: BY Roel Cobarde M.DMiriam JonesNo ratings yet
- Introduction to Osteology: Bones and Skeletal AnatomyDocument29 pagesIntroduction to Osteology: Bones and Skeletal AnatomyANN MARIYA MONCYNo ratings yet
- Beka Aroshidze 2017Document48 pagesBeka Aroshidze 2017Rupesh M DasNo ratings yet
- General AnatomyDocument17 pagesGeneral AnatomyAbubakar Umar GaladanchiNo ratings yet
- Understanding the Structure and Function of Bones and JointsDocument36 pagesUnderstanding the Structure and Function of Bones and JointsBenedict BuitizonNo ratings yet
- Concept 3 Notes - Anatomy Basics For StudentsDocument39 pagesConcept 3 Notes - Anatomy Basics For StudentsKaranNo ratings yet
- Introduction To The Anatomy,: Sagittal PlaneDocument10 pagesIntroduction To The Anatomy,: Sagittal PlanemagholNo ratings yet
- The Skeletal System: Bones, Joints and Functions in 40 CharactersDocument61 pagesThe Skeletal System: Bones, Joints and Functions in 40 Charactersdrin zekaNo ratings yet
- المحاضرة الثانية تشريح اسنان م 1Document26 pagesالمحاضرة الثانية تشريح اسنان م 1mfhrluvxxxNo ratings yet
- Anatomy (302) - 1Document82 pagesAnatomy (302) - 1Shehzad Noman SajidNo ratings yet
- IntroductionDocument64 pagesIntroductionkarokamil243No ratings yet
- HSB Week 13Document19 pagesHSB Week 13edhanassarNo ratings yet
- Intro To Diagnostic Imaging - 2 - Prof - Dr.i̇smet TAMERDocument37 pagesIntro To Diagnostic Imaging - 2 - Prof - Dr.i̇smet TAMERAly MssreNo ratings yet
- Lec.2 Introduction Anatomy PDFDocument34 pagesLec.2 Introduction Anatomy PDFKhadija KadhimNo ratings yet
- Premedical Biology: Motor MechanismDocument44 pagesPremedical Biology: Motor MechanismsheenaNo ratings yet
- Skeletal System (2) - 2Document71 pagesSkeletal System (2) - 2alazarademe797No ratings yet
- Muscle, Structure, and FunctionDocument59 pagesMuscle, Structure, and FunctionJesus AbgNo ratings yet
- Skeletal System FrameworkDocument82 pagesSkeletal System FrameworkJexine YsabelleNo ratings yet
- The Human Anatomy & PhysiologyDocument22 pagesThe Human Anatomy & PhysiologyAditya VijayNo ratings yet
- GROSS ANATOMY I OVERVIEWDocument274 pagesGROSS ANATOMY I OVERVIEWNadim KhadkaNo ratings yet
- Anatomy and PhysiologyDocument65 pagesAnatomy and PhysiologyJosef BaroniNo ratings yet
- Anatomy and Physiology LectrueDocument76 pagesAnatomy and Physiology LectrueButch Dumdum73% (15)
- Muscles: Dr. Maung MyintDocument54 pagesMuscles: Dr. Maung MyintIntan AinNo ratings yet
- Anatomy and Physiology of Farm AnimalsDocument262 pagesAnatomy and Physiology of Farm AnimalsSuShi-sunIñigoNo ratings yet
- Embryology: Abdulrahman Uday AbdulfatahDocument27 pagesEmbryology: Abdulrahman Uday AbdulfatahAbdulrahman UdayNo ratings yet
- The Skeletal SystemDocument30 pagesThe Skeletal SystemFAtma HAnysNo ratings yet
- Skeletalsystem MRDDocument35 pagesSkeletalsystem MRDArnold Ashish GomesNo ratings yet
- Anatomy Week 3 NotesDocument32 pagesAnatomy Week 3 NotesBasil AdeelNo ratings yet
- L2 Body StructuresDocument8 pagesL2 Body Structureszabdullahstud1No ratings yet
- Intro To Ortho Anatomy PDFDocument55 pagesIntro To Ortho Anatomy PDFlanghalilafaNo ratings yet
- Anatomy U-3 Skeletal SystemDocument109 pagesAnatomy U-3 Skeletal Systemsinte beyuNo ratings yet
- Ilovepdf Merged 1 13Document13 pagesIlovepdf Merged 1 13Abdulrahman UdayNo ratings yet
- Human Movement and Bones: Ms. Marcheli Alexandra, S.PD Junior High Sekolah Global Mandiri Cibubur 2018-2019Document19 pagesHuman Movement and Bones: Ms. Marcheli Alexandra, S.PD Junior High Sekolah Global Mandiri Cibubur 2018-2019Andy WarholNo ratings yet
- Group2 - BSHM 1 BDocument43 pagesGroup2 - BSHM 1 BSAPILAN DENMARNo ratings yet
- Musculoskeletal System SummaryDocument7 pagesMusculoskeletal System SummaryFuzna DahliaNo ratings yet
- Joints of The Head and Trunk - 2015-RuanDocument30 pagesJoints of The Head and Trunk - 2015-RuanKw ChanNo ratings yet
- Medical Surgical Nursing OrthopedicDocument22 pagesMedical Surgical Nursing Orthopedicroger80% (5)
- 1.introduction To AnatomyDocument30 pages1.introduction To AnatomyDixonLing100% (1)
- Anatomical IntroductionDocument17 pagesAnatomical Introductionllazoozllbraa 7372No ratings yet
- (Oct 1) THE SKELETAL SYSTEM PDFDocument7 pages(Oct 1) THE SKELETAL SYSTEM PDFBea GualbertoNo ratings yet
- Skeletal and Muscular Systems ExplainedDocument20 pagesSkeletal and Muscular Systems ExplainedTuaha MasoodNo ratings yet
- Prof. Dr. Dr. Yanwirasti, Pa (K)Document143 pagesProf. Dr. Dr. Yanwirasti, Pa (K)bibleeNo ratings yet
- The Muscular System ExplainedDocument22 pagesThe Muscular System ExplainedFiraol DiribaNo ratings yet
- Overview of The Musculoskeletal System: For Year 1 Medicine By: Zelalem.aDocument36 pagesOverview of The Musculoskeletal System: For Year 1 Medicine By: Zelalem.aAmanuel MaruNo ratings yet
- Hs 2Document5 pagesHs 2Elyka Alivan Valdez PolonioNo ratings yet
- PDS01A- Lesson 1Document30 pagesPDS01A- Lesson 1aresfenrirNo ratings yet
- Muscular SystemDocument26 pagesMuscular Systemlubnab67% (3)
- Introduction To AnatomyDocument9 pagesIntroduction To AnatomyFoo FuuNo ratings yet
- Introduction To Veterinary AnatomyDocument118 pagesIntroduction To Veterinary AnatomyKhrys Hardy100% (1)
- Musculoskeletal System-Topic 8Document40 pagesMusculoskeletal System-Topic 8Heba TabchNo ratings yet
- 1st Week - Introduction To AnatomyDocument32 pages1st Week - Introduction To AnatomyyazicigaamzeNo ratings yet
- Anatomy IntrodactionDocument48 pagesAnatomy IntrodactionYasin AbassNo ratings yet
- Introduction To Body StructureDocument34 pagesIntroduction To Body StructureBrady DeNioNo ratings yet
- 2.0 Tissues and Supporting SystemDocument39 pages2.0 Tissues and Supporting Systemwalterkalu385No ratings yet
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument10 pagesOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreYoAmoNYC100% (1)
- Anatomy for Artists: A Complete Guide to Drawing the Human BodyFrom EverandAnatomy for Artists: A Complete Guide to Drawing the Human BodyRating: 3 out of 5 stars3/5 (3)
- Drawing Anatomy: An Artist's Guide to the Human FigureFrom EverandDrawing Anatomy: An Artist's Guide to the Human FigureRating: 3 out of 5 stars3/5 (1)
- Radiographic Positioning and Related Anatomy 8th Edition Bontrager Test BankDocument25 pagesRadiographic Positioning and Related Anatomy 8th Edition Bontrager Test BankGaryDavisfdzb100% (39)
- Advanced Assessment Chest Assessment and Auscultation: Base Hospital GroupDocument41 pagesAdvanced Assessment Chest Assessment and Auscultation: Base Hospital GroupdeebertoNo ratings yet
- Breathing and Exchange of GasesDocument25 pagesBreathing and Exchange of GasesSureshNo ratings yet
- Anatomy & Physiology (Chapter 1 - The Human Organism)Document23 pagesAnatomy & Physiology (Chapter 1 - The Human Organism)Ellie EileithyiaNo ratings yet
- Chest - Internal Medicine, Dr. A. Mowafy (2020-2021) .Document193 pagesChest - Internal Medicine, Dr. A. Mowafy (2020-2021) .Mohammed Risq67% (3)
- 2020 - BPT Obe Syllabus-1Document282 pages2020 - BPT Obe Syllabus-1Akshaya MistryNo ratings yet
- Differential Diagnosis BookDocument101 pagesDifferential Diagnosis BookAmanda PratiwiNo ratings yet
- O CO O CO O CO: Chapter 15: Respiratory SystemDocument3 pagesO CO O CO O CO: Chapter 15: Respiratory SystemPrecious Faith RodriguezNo ratings yet
- Chapter 3Document54 pagesChapter 3Ayro Business CenterNo ratings yet
- Black Book PDFDocument464 pagesBlack Book PDFHeba100% (1)
- Parts of Resperatory SystemDocument5 pagesParts of Resperatory SystemPeysbukan Cyber CafeNo ratings yet
- Pleural Effusion - Imaging AdultsDocument58 pagesPleural Effusion - Imaging AdultsAlienNo ratings yet
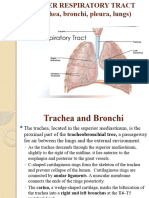
- Lower Resp TractDocument32 pagesLower Resp TractTakshikaNo ratings yet
- Detecting Heartbeats and Diagnosing Chest PainDocument113 pagesDetecting Heartbeats and Diagnosing Chest PainNasan Shehada100% (1)
- Chest Tube Manual Atrium Green HandbookDocument40 pagesChest Tube Manual Atrium Green HandbookprogramgrabberNo ratings yet
- Penetrating Trauma CheatsheetDocument3 pagesPenetrating Trauma Cheatsheetdruhh100% (1)
- Deposition, Clearance, and Translocation of Chrysotile Asbestos From Peripheral and Central Regions of The Rat LungDocument20 pagesDeposition, Clearance, and Translocation of Chrysotile Asbestos From Peripheral and Central Regions of The Rat LungKhambang AirlanggaNo ratings yet
- Physics of RadiologyDocument9 pagesPhysics of RadiologyChristian PasicolanNo ratings yet
- Unit 3 Anatomy of Respiratory System: External Respiration. The Exchange of Gases Between The Blood in The Capillaries ofDocument35 pagesUnit 3 Anatomy of Respiratory System: External Respiration. The Exchange of Gases Between The Blood in The Capillaries ofAnne RonquilloNo ratings yet
- Human Physiology 01 - Theory Notes - PDF Only - NSEJS 2023Document94 pagesHuman Physiology 01 - Theory Notes - PDF Only - NSEJS 2023Chinmay GoelNo ratings yet
- Anatomy and Physiology LectrueDocument76 pagesAnatomy and Physiology LectrueButch Dumdum73% (15)
- The Anatomy of the ThoraxDocument237 pagesThe Anatomy of the ThoraxAbel Belete100% (1)
- Respiratory PhysiologyDocument37 pagesRespiratory PhysiologyGuillermo Sasso Pacheco100% (1)
- Lungs-WPS OfficeDocument23 pagesLungs-WPS Officezenith parmarNo ratings yet
- Recognition, Diagnosis and Treatment of Pneumothorax, Hemothorax and Chest TraumaDocument59 pagesRecognition, Diagnosis and Treatment of Pneumothorax, Hemothorax and Chest TraumaAnusha VergheseNo ratings yet
- Respiratory Notes and SlideDocument33 pagesRespiratory Notes and SlideChristina Gonez100% (1)
- Chapter 022Document32 pagesChapter 022Nur SusiawantyNo ratings yet
- Thoracos PDFDocument40 pagesThoracos PDFmanjunath kalal100% (1)
- Disorder of Respiratory SystemDocument89 pagesDisorder of Respiratory SystemDarine NasrNo ratings yet
- 1-Snell's Clinical Anatomy by Regions 9th 2012Document44 pages1-Snell's Clinical Anatomy by Regions 9th 2012Jeane Irish Paller EgotNo ratings yet