You might also like
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
- Technology in Practical Dermatology: Non-Invasive Imaging, Lasers and Ulcer ManagementFrom EverandTechnology in Practical Dermatology: Non-Invasive Imaging, Lasers and Ulcer ManagementMichele FimianiNo ratings yet
- LOCAL ANESTHETICS MECHANISMDocument30 pagesLOCAL ANESTHETICS MECHANISMCorry QyNo ratings yet
- ANS ReceptorsDocument14 pagesANS ReceptorsAisha AliNo ratings yet
- Pathophysiology Prof PlevkovaDocument414 pagesPathophysiology Prof PlevkovaPrince XavierNo ratings yet
- Pharmacology Module PDFDocument23 pagesPharmacology Module PDFmirza_baig_46100% (1)
- Chapter 43 - Beta-LactamDocument7 pagesChapter 43 - Beta-LactamErika De JesusNo ratings yet
- Mu 002Document10 pagesMu 002chandanNo ratings yet
- Revellionz'19 - Second Year Question BankDocument114 pagesRevellionz'19 - Second Year Question BankRamNo ratings yet
- Antibiotics 9Document11 pagesAntibiotics 9Beth Morales100% (1)
- Drug InteractionsDocument33 pagesDrug Interactions88AKK100% (1)
- AntiemeticsDocument25 pagesAntiemeticsPridho GaziansyahNo ratings yet
- PharmecogenomicsDocument21 pagesPharmecogenomicsRatan Ratan100% (1)
- Basic Concept of General AnesthesiaDocument97 pagesBasic Concept of General Anesthesiasanjivdas100% (1)
- Surgical Antibiotic ProphylaxisDocument7 pagesSurgical Antibiotic ProphylaxisRony Rony100% (1)
- Anti-infective Agents Chapter OverviewDocument13 pagesAnti-infective Agents Chapter OverviewEricka AbellaNo ratings yet
- Arthroplasty JournalDocument3 pagesArthroplasty Journallina yohanes100% (1)
- ChemotherapyDocument11 pagesChemotherapyNedaAbdullahNo ratings yet
- Fungal Infections of Oral Cavity: Diagnosis, Management, and Association With COVID-19Document12 pagesFungal Infections of Oral Cavity: Diagnosis, Management, and Association With COVID-19Roxana Guerrero SoteloNo ratings yet
- Cardiovascular PharmacologyDocument61 pagesCardiovascular PharmacologyTeeOne920% (1)
- Acetylcholine and Autonomic DrugsDocument20 pagesAcetylcholine and Autonomic DrugsPrincess Mara DuranNo ratings yet
- Histamine and Antihistamines. NotesDocument5 pagesHistamine and Antihistamines. NotesSubha2000100% (1)
- Anti EmeticsDocument29 pagesAnti EmeticsBezawit Tsige100% (1)
- Anti-Viral Drugs AltDocument42 pagesAnti-Viral Drugs AltSidraNo ratings yet
- Tmd175 Slide Pharmacology of Antifungi Anthelminthics AntiprotozoalDocument38 pagesTmd175 Slide Pharmacology of Antifungi Anthelminthics AntiprotozoalYeni SuwitaNo ratings yet
- Pharmacology Quick HitsDocument6 pagesPharmacology Quick HitsHuma Hameed DogarNo ratings yet
- Vancomycin Pharmacology Indications, Mechanism, and Side Effects! PDFDocument1 pageVancomycin Pharmacology Indications, Mechanism, and Side Effects! PDFFrancis PasayNo ratings yet
- 10 Pharmacology - ImmunopharmacologyDocument17 pages10 Pharmacology - ImmunopharmacologyArnoldBorromeoNo ratings yet
- Drug Suffixes and Their MeaningsDocument3 pagesDrug Suffixes and Their MeaningsSharon TanveerNo ratings yet
- Rational Use of Antibiotics STDocument32 pagesRational Use of Antibiotics STArita Rahmadarni100% (1)
- Pharmacology of The GITDocument31 pagesPharmacology of The GITmarviecute22No ratings yet
- Pharmacology AntibioticsDocument70 pagesPharmacology Antibioticsmaggie100% (1)
- Drugs Acting On The AnsDocument57 pagesDrugs Acting On The AnsAnonymous iG0DCOfNo ratings yet
- Quinolones, Folic Acid Antagonist and Urinary Tract Antitb and LeprosyDocument124 pagesQuinolones, Folic Acid Antagonist and Urinary Tract Antitb and LeprosyrenNo ratings yet
- Pharmacology of Drugs Used in Bronchial Asthma & COPDDocument84 pagesPharmacology of Drugs Used in Bronchial Asthma & COPDdfngjlnNo ratings yet
- Autacoids: Group No. 1Document92 pagesAutacoids: Group No. 1Rohan Pal100% (1)
- Arrhythmia Drugs Test QuestionsDocument7 pagesArrhythmia Drugs Test QuestionsDrishya BioplannetNo ratings yet
- Katzung & Trevor's Pharmacology Examination & Board Review-Pages-303-311Document9 pagesKatzung & Trevor's Pharmacology Examination & Board Review-Pages-303-311Princess Alyssa H. PasajolNo ratings yet
- AntibioticsDocument39 pagesAntibioticsmekaiel100% (2)
- Pharmacology notes on adrenergic agonists and antagonistsDocument3 pagesPharmacology notes on adrenergic agonists and antagonistsMohd Afiq AizuddinNo ratings yet
- Pharma 1.2 - Pharmacokinetics (Wini Ong) PDFDocument11 pagesPharma 1.2 - Pharmacokinetics (Wini Ong) PDFVon Javier GamateroNo ratings yet
- PCP - Doctors' RightsDocument26 pagesPCP - Doctors' RightsianNo ratings yet
- Protein Synthesis InhibitorsDocument58 pagesProtein Synthesis InhibitorsmulatumeleseNo ratings yet
- Pharmacodynamics 4Document28 pagesPharmacodynamics 4علي المحترفNo ratings yet
- Morphologic Patterns of Acute InflammationDocument51 pagesMorphologic Patterns of Acute Inflammationحفصه حسينNo ratings yet
- CNS-Classifications by Dr-Islahkhan (Humble Pharmacist)Document24 pagesCNS-Classifications by Dr-Islahkhan (Humble Pharmacist)M Ils Meteor Pharmacist0% (1)
- Arthritis BrexDocument48 pagesArthritis BrexKate EvangelistaNo ratings yet
- Chemotherapy NDocument28 pagesChemotherapy NFaisal MehboobNo ratings yet
- Drugs for Cough, Bronchial Asthma and InflammationDocument47 pagesDrugs for Cough, Bronchial Asthma and InflammationNavlika DuttaNo ratings yet
- AutacoidsDocument32 pagesAutacoidsRenellie TrimidalNo ratings yet
- CNS Depressants and Muscle RelaxantsDocument23 pagesCNS Depressants and Muscle RelaxantsSV SagarNo ratings yet
- Antibiotics Training ManualDocument149 pagesAntibiotics Training ManualImran MullaNo ratings yet
- Antibiotic Prophylaxis PDFDocument3 pagesAntibiotic Prophylaxis PDFPadmanabha GowdaNo ratings yet
- Rational Use of AntibioticsDocument32 pagesRational Use of AntibioticsRendy SusantoNo ratings yet
- Oral Path Case Study PaperDocument4 pagesOral Path Case Study PaperSukirti MisraNo ratings yet
- 9autacoids 14010v9023022 Phpapp02Document109 pages9autacoids 14010v9023022 Phpapp02h3cn1r3100% (1)
- LIGAND - Receptors Concept FKG 2012 Univ YarsiDocument29 pagesLIGAND - Receptors Concept FKG 2012 Univ Yarsidayanara_245104654No ratings yet
- Drug Interactions of Antianginal Drugs..Document40 pagesDrug Interactions of Antianginal Drugs..Kamal SikandarNo ratings yet
- Clinical Pharmacology: Proceedings of the 7th International Congress of Pharmacology, Paris 1978From EverandClinical Pharmacology: Proceedings of the 7th International Congress of Pharmacology, Paris 1978P. Duchêne-MarullazNo ratings yet
- Therapeutic Hypothermia - Principles, Indications, Practical ApplicationFrom EverandTherapeutic Hypothermia - Principles, Indications, Practical ApplicationNo ratings yet
- Abortus WilliamDocument77 pagesAbortus WilliamDesmy AdeliaNo ratings yet
- The GlaucomasDocument29 pagesThe GlaucomasJk FloresNo ratings yet
- 1 New 2010 Bls For Healthcare Worker OkDocument50 pages1 New 2010 Bls For Healthcare Worker OkJulienne CaoileNo ratings yet
- Cesarean Delivery and HysterectomyDocument68 pagesCesarean Delivery and HysterectomyJk FloresNo ratings yet
- Chronic Renal FailureDocument58 pagesChronic Renal FailureJk FloresNo ratings yet
- Anatomy Mcqs With AnswersDocument8 pagesAnatomy Mcqs With AnswersJk Flores67% (6)
- ARTHRITISDocument4 pagesARTHRITISJk FloresNo ratings yet
- Metabolic Bone DiseasesDocument55 pagesMetabolic Bone DiseasesJk FloresNo ratings yet
- Popliteal Fossa 1Document2 pagesPopliteal Fossa 1Jk FloresNo ratings yet
- Larynx LectureffDocument30 pagesLarynx Lectureffmohidul25No ratings yet
- Syllabus For Third Year Allied Health Science Courses AOTDocument10 pagesSyllabus For Third Year Allied Health Science Courses AOTAnil KumarNo ratings yet
- DAFTAR OBAT AMAN DAN BERBAHAYA UNTUK IBU HAMIL DAN MENYUSUIDocument30 pagesDAFTAR OBAT AMAN DAN BERBAHAYA UNTUK IBU HAMIL DAN MENYUSUIMuharramNo ratings yet
- Inhalation AnestheticsDocument27 pagesInhalation AnestheticsMarcelitaTaliaDuwiriNo ratings yet
- AnestheticsDocument32 pagesAnestheticsAnkit JainNo ratings yet
- Anesthesia-Induced Immune Modulation: ReviewDocument7 pagesAnesthesia-Induced Immune Modulation: ReviewFIA SlotNo ratings yet
- Must Know 151 Topics - NeetPG PYT List.Document71 pagesMust Know 151 Topics - NeetPG PYT List.Kamal SinghNo ratings yet
- Rocuronium: Bromide InjectionDocument2 pagesRocuronium: Bromide InjectionNursalfarinah BasirNo ratings yet
- A Review of The Physiological Effects of 2-Agonists Small Animal PraticeDocument13 pagesA Review of The Physiological Effects of 2-Agonists Small Animal PraticeMabe AguirreNo ratings yet
- Local AnesthesiaDocument40 pagesLocal AnesthesiaKY HoNo ratings yet
- Webinar On Canine Anaesthesia Under Field Condition 17 05 2020Document87 pagesWebinar On Canine Anaesthesia Under Field Condition 17 05 2020hari krishnaa athotaNo ratings yet
- Anesthesia: Ucsd Institutional Animal Care and Use Committee Policy Manual POLICY 34.06Document10 pagesAnesthesia: Ucsd Institutional Animal Care and Use Committee Policy Manual POLICY 34.06Ahmad HendawiNo ratings yet
- Chapter ReviewDocument32 pagesChapter ReviewThanh TrúcNo ratings yet
- The Medical Student's Guide to AnesthesiaDocument16 pagesThe Medical Student's Guide to Anesthesiamarianaalvim100% (1)
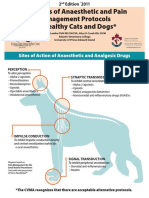
- Examples of Anaesthetic and Pain Management Protocols For Healthy Cats and DogsDocument3 pagesExamples of Anaesthetic and Pain Management Protocols For Healthy Cats and DogsEka FirmanNo ratings yet
- PHARMACOLOGY OVERVIEWDocument67 pagesPHARMACOLOGY OVERVIEWZehra KhanNo ratings yet
- Management of Local Anaesthetic Toxicity Update 2009Document6 pagesManagement of Local Anaesthetic Toxicity Update 2009leviosagalNo ratings yet
- 2009-07-31 Animal Shelter ManualDocument38 pages2009-07-31 Animal Shelter ManualEwing Township, NJ100% (2)
- Anaesthesia by Joe Agyeman-1Document35 pagesAnaesthesia by Joe Agyeman-1Michael AdjeiNo ratings yet
- Drugs Acting On The Central Nervous System (21) Subcommittee: NameDocument19 pagesDrugs Acting On The Central Nervous System (21) Subcommittee: NameahmadyasinhavidNo ratings yet
- Precedex Dosing GuidelinesDocument15 pagesPrecedex Dosing GuidelinesemonhalimNo ratings yet
- General Anesthesia: Presented By: Shalakha Bhardwaj BDS Final Year (2007-2011)Document85 pagesGeneral Anesthesia: Presented By: Shalakha Bhardwaj BDS Final Year (2007-2011)KrishnaBihariShuklaNo ratings yet
- 4 5774036780135220376 PDFDocument102 pages4 5774036780135220376 PDFAhmed Fikry100% (2)
- Delayed Awakening From AnaesthesiaDocument3 pagesDelayed Awakening From AnaesthesiaSenthooran ArudshivsmNo ratings yet
- Anesthesia For Thymectomy 222Document62 pagesAnesthesia For Thymectomy 222drchandrus100% (1)
- Anaesthesia For Non-Obstetric Surgery During Pregnancy: Review ArticleDocument8 pagesAnaesthesia For Non-Obstetric Surgery During Pregnancy: Review ArticleFemiko Panji AprilioNo ratings yet
- Peri Operative NursingDocument22 pagesPeri Operative NursingIvyBanez100% (1)
- WHOModelFormulary - Children 94 PDFDocument528 pagesWHOModelFormulary - Children 94 PDFCristianJiménezNo ratings yet
- Management of Life-Threatening Asthma (@ eDocument10 pagesManagement of Life-Threatening Asthma (@ eLex X PabloNo ratings yet
- Smith's Anesthesia For Infants and ChildrenDocument17 pagesSmith's Anesthesia For Infants and ChildrenRamos Zavala Julio CesarNo ratings yet
- BJAS - Volume 5 - Issue Issue 1 Part (2) - Pages 275-281Document7 pagesBJAS - Volume 5 - Issue Issue 1 Part (2) - Pages 275-281Vengky UtamiNo ratings yet