You might also like
- Module 3 HA Comprehensive Health History 1Document16 pagesModule 3 HA Comprehensive Health History 1Rosalinda LacuestaNo ratings yet
- The Complete Health History Grup 1Document19 pagesThe Complete Health History Grup 1Nadia MulyaNo ratings yet
- Nursing History Form and SampleDocument3 pagesNursing History Form and SampleRalph Laurence TanNo ratings yet
- History Taking2Document25 pagesHistory Taking2Capture UnseenNo ratings yet
- Tehnik Penyusunan Status Penderita BedahDocument30 pagesTehnik Penyusunan Status Penderita BedahsimcassNo ratings yet
- FolletoDocument10 pagesFolletoLuis Angel BejeranoNo ratings yet
- Adult Physical AssessmentDocument18 pagesAdult Physical AssessmentHa HahahahahaNo ratings yet
- Nursing History - A. Syanthiqah TirtaDocument3 pagesNursing History - A. Syanthiqah TirtaSanti TirtaNo ratings yet
- Ealth History:: Collecting Data HDocument10 pagesEalth History:: Collecting Data HCindz De CastroNo ratings yet
- History Taking in MedicineDocument14 pagesHistory Taking in MedicineRaman Prasad SharmaNo ratings yet
- Health HistoryDocument7 pagesHealth HistoryAnnapurna DangetiNo ratings yet
- PEDIA 1 The Pediatric History and Physical Exam HandoutDocument16 pagesPEDIA 1 The Pediatric History and Physical Exam HandoutRyan Loyd MarquezNo ratings yet
- History Taking and PEDocument30 pagesHistory Taking and PEMelissa Salayog100% (1)
- 第一次课history-taking - 瞿立辉 2.29Document88 pages第一次课history-taking - 瞿立辉 2.29Mar ClrNo ratings yet
- Mustansiriyah Lecture Notes On Surgical History & Clinical ExaminationDocument57 pagesMustansiriyah Lecture Notes On Surgical History & Clinical Examinationنور الهدى ابراهيم خضير معيليNo ratings yet
- History Taking SkillsDocument39 pagesHistory Taking Skillschifunndo charlesNo ratings yet
- Comprehensive Respiratory InterviewDocument36 pagesComprehensive Respiratory InterviewDharlyn MungcalNo ratings yet
- Endocrine OsceDocument11 pagesEndocrine OsceLesego Ladylee ManokoNo ratings yet
- NCM-101-Lecture-2 (1)Document217 pagesNCM-101-Lecture-2 (1)Jane Heart AguilonNo ratings yet
- Class: 4-C of Nursing Aprillia Nurul (201502082) Destiana P. (201502086)Document12 pagesClass: 4-C of Nursing Aprillia Nurul (201502082) Destiana P. (201502086)APRILIA NURULNo ratings yet
- Complete Health HistoryDocument22 pagesComplete Health HistorykhalidNo ratings yet
- Pediatric vs Adult Patient DifferencesDocument7 pagesPediatric vs Adult Patient DifferencesabhivnairNo ratings yet
- Clinical Case Presentations CARE IIDocument44 pagesClinical Case Presentations CARE IIStarr Newman100% (1)
- 02 C F Components of HistoryDocument34 pages02 C F Components of HistoryYared TJNo ratings yet
- Examining the Cardiovascular SystemDocument152 pagesExamining the Cardiovascular SystemAloah122346100% (2)
- 2beginning The History Taking-1Document30 pages2beginning The History Taking-1Wizz Háķìm ĻêşòwNo ratings yet
- Emedley Practice/ Guidelines: JaniceDocument13 pagesEmedley Practice/ Guidelines: JaniceRupsyNo ratings yet
- History Taking Physical ExamininationDocument41 pagesHistory Taking Physical ExamininationAya AmerNo ratings yet
- Pendekatan Pada Pasien Anak (anamnesis+PF)Document25 pagesPendekatan Pada Pasien Anak (anamnesis+PF)Sarah AgustinNo ratings yet
- 2.4 (Mfa) Examination of The PatientDocument6 pages2.4 (Mfa) Examination of The PatientTEY NuwansaraNo ratings yet
- Baker PediatricsHist02Document11 pagesBaker PediatricsHist02Ben DavidNo ratings yet
- Case Study Elective1Document32 pagesCase Study Elective1Jhem SiribanNo ratings yet
- 7lab 2 FCM IDocument13 pages7lab 2 FCM Iparanoea911No ratings yet
- Patient Examination: History: by Professor of Internal MedicineDocument47 pagesPatient Examination: History: by Professor of Internal MedicineMonqith YousifNo ratings yet
- History & Physical Diagnostic#Document106 pagesHistory & Physical Diagnostic#Olsa Alshapira100% (1)
- History & Physical ExaminationDocument67 pagesHistory & Physical ExaminationDiggi VioNo ratings yet
- 1) Identification Data:: Guide For Taking History in PediatricsDocument5 pages1) Identification Data:: Guide For Taking History in PediatricsAhmed Mansor AlariqiNo ratings yet
- Patient Assessment FormDocument8 pagesPatient Assessment Formjerickpacia2000No ratings yet
- Foundations of Clinical Medicine-1 Summer 2014 Semester: History TakingDocument63 pagesFoundations of Clinical Medicine-1 Summer 2014 Semester: History Takingparanoea911100% (1)
- 15.1. History Taking + ECG 1-肖培林Document125 pages15.1. History Taking + ECG 1-肖培林mirabel IvanaliNo ratings yet
- Diagnostic of Internal Diseases. Main Methods of Examination. Lecture N1Document40 pagesDiagnostic of Internal Diseases. Main Methods of Examination. Lecture N1Noor AliNo ratings yet
- Chapter One Introduction To Clinical MedicineDocument23 pagesChapter One Introduction To Clinical MedicinemulaewolloNo ratings yet
- Shelf IM Patient NotesDocument6 pagesShelf IM Patient NotesRuth SanmooganNo ratings yet
- HistoryDocument27 pagesHistoryabuhajerah15No ratings yet
- Pom MidtermsDocument692 pagesPom MidtermsGwyneth MendozaNo ratings yet
- Recording The Medical HistoryDocument8 pagesRecording The Medical HistorypasambalyrradjohndarNo ratings yet
- Pediatric Case ApproachDocument47 pagesPediatric Case ApproachKenneth NuñezNo ratings yet
- Nsg241 Study Guide Exam 5Document76 pagesNsg241 Study Guide Exam 5NatalieAndersonNo ratings yet
- Stress Insomnia OutputDocument18 pagesStress Insomnia OutputReyes PaulNo ratings yet
- Health AssessmentDocument31 pagesHealth AssessmentLoi Ocampo Crespo100% (1)
- Outline For Pediatric History and Physical Examination History I. Presenting Complaint (Informant/Reliability of Informant)Document4 pagesOutline For Pediatric History and Physical Examination History I. Presenting Complaint (Informant/Reliability of Informant)Hawkar SaeedNo ratings yet
- Taking A Health History Health History: PurposeDocument17 pagesTaking A Health History Health History: PurposeKaye CorNo ratings yet
- Nursing Health HistoryDocument45 pagesNursing Health HistoryCatlyn Chatpman100% (1)
- The Format: Case Study FormDocument17 pagesThe Format: Case Study FormJane DyNo ratings yet
- History Taking Guide - 70% Diagnosis from Patient HistoryDocument51 pagesHistory Taking Guide - 70% Diagnosis from Patient HistoryJAMES TONNY OKINYINo ratings yet
- History Taking - The Critical First Step in DiagnosisDocument51 pagesHistory Taking - The Critical First Step in DiagnosisJAMES TONNY OKINYINo ratings yet
- Health Assessment SAS Session 2Document5 pagesHealth Assessment SAS Session 2Mary Maxiluch TabudlongNo ratings yet
- Anamnesis: (Recollection, A Patient Case History)Document13 pagesAnamnesis: (Recollection, A Patient Case History)AlbertoKosasihNo ratings yet
- Barriers To Communication: Communication Barrier - Anything That Gets in The Way of Clear CommunicationDocument29 pagesBarriers To Communication: Communication Barrier - Anything That Gets in The Way of Clear CommunicationRana Waji Ul HassanNo ratings yet
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
- Fourmula One For HealthDocument19 pagesFourmula One For HealthAlbert B. BalaceNo ratings yet
- Fourmula One For HealthDocument19 pagesFourmula One For HealthAlbert B. BalaceNo ratings yet
- Neurological AssessmentDocument53 pagesNeurological AssessmentAlbert B. BalaceNo ratings yet
- Elder AbuseDocument53 pagesElder AbuseAlbert B. Balace100% (1)
- Neurological AssessmentDocument53 pagesNeurological AssessmentAlbert B. BalaceNo ratings yet
- PHC 2Document31 pagesPHC 2Albert B. BalaceNo ratings yet
- Indigenous Fermented Food and BeveragesDocument5 pagesIndigenous Fermented Food and BeveragesdodecadidoNo ratings yet
- Biyahe Ni Drew - BatangasDocument9 pagesBiyahe Ni Drew - BatangasJohn JerichoNo ratings yet
- Friederich Gualdus Revelation of The True Chemical WisdomDocument30 pagesFriederich Gualdus Revelation of The True Chemical WisdomtravellerfellowNo ratings yet
- USBN 2018-2019 English Exam Practice QuestionsDocument10 pagesUSBN 2018-2019 English Exam Practice QuestionsauleeahgittaNo ratings yet
- ORGAN CULTURE, Anther & Pollen CultureDocument72 pagesORGAN CULTURE, Anther & Pollen CultureSanthiyaNo ratings yet
- Exu & Maria Padilla Reina List of HerbsDocument2 pagesExu & Maria Padilla Reina List of HerbsGnostic the Ancient OneNo ratings yet
- 11 Umiami - Series A PitchdeckDocument21 pages11 Umiami - Series A PitchdeckCastille BrousseNo ratings yet
- Experience Dominica 2014Document96 pagesExperience Dominica 2014eWIPWorldNo ratings yet
- Bài Tập Câu Điều KiệnDocument4 pagesBài Tập Câu Điều KiệnHương100% (1)
- Soal Pas Gasal Grow With English 2Document3 pagesSoal Pas Gasal Grow With English 2LuthfiBurhanandaNo ratings yet
- P.MKT Dawn BreadDocument36 pagesP.MKT Dawn BreadShaikhNo ratings yet
- Lesson PlanDocument3 pagesLesson Planapi-253745878No ratings yet
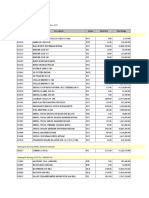
- LAPORAN RATA-RATA HARGA BELIDocument315 pagesLAPORAN RATA-RATA HARGA BELIfadjaroeddinNo ratings yet
- Redefining Security - Richard UllmanDocument26 pagesRedefining Security - Richard UllmanFaig Abbasov100% (1)
- DualityDocument91 pagesDualityმარი ლელუაშვილიNo ratings yet
- M4-L2 Information ArchitectureDocument66 pagesM4-L2 Information ArchitectureAnonymous 7PmasFlc6yNo ratings yet
- Making Sense of TasteDocument10 pagesMaking Sense of TastetufekciosmanNo ratings yet
- aaaaaaaaaaaaaaaaaaaaaaaaaaaDLL - SCIENCE 5 - Q1 - W6Document10 pagesaaaaaaaaaaaaaaaaaaaaaaaaaaaDLL - SCIENCE 5 - Q1 - W6Jsm JsmNo ratings yet
- Buff ColorationDocument273 pagesBuff ColorationJan Frederik Valkenberg CastroNo ratings yet
- (CD8) Cum Tu Co Dinh Tuan 16 128556 220202250340PMDocument17 pages(CD8) Cum Tu Co Dinh Tuan 16 128556 220202250340PMKieu An HoangNo ratings yet
- YANMart Tangerang Purchase Order Provides Details of Various Food and Beverage ProductsDocument4 pagesYANMart Tangerang Purchase Order Provides Details of Various Food and Beverage ProductsIndoflac MusicNo ratings yet
- Answer Sheet: First Quarter Module 9 (Lesson 2) Benefits That Cab Be Derived From Animal/Fish RaisingDocument1 pageAnswer Sheet: First Quarter Module 9 (Lesson 2) Benefits That Cab Be Derived From Animal/Fish RaisingLorinda De Lara GonzaloNo ratings yet
- Spanish TapasDocument8 pagesSpanish TapasMarta vasquezNo ratings yet
- People: Watch The Video Podcast. Which Person's Life Is Similar To Yours?Document5 pagesPeople: Watch The Video Podcast. Which Person's Life Is Similar To Yours?Hugo TrejoNo ratings yet
- Module 3Document3 pagesModule 3Cherry Ann Joy AbonNo ratings yet
- Integrated Rice and Duck Farming - Takao Furuno CaseDocument2 pagesIntegrated Rice and Duck Farming - Takao Furuno CaseRija Ménagé100% (1)
- Macaroni Salad RecipeDocument12 pagesMacaroni Salad RecipePrince Louie MorteNo ratings yet
- Access 2 VocabularyDocument5 pagesAccess 2 VocabularyAlexandra Sandra KalevraNo ratings yet
- Calculus 10th Edition Larson Test Bank 1Document36 pagesCalculus 10th Edition Larson Test Bank 1bonniewilsoncqpkszdmgj100% (22)
- b676 Boysen Quick Drying Enamel OrangeDocument10 pagesb676 Boysen Quick Drying Enamel OrangeMike Advincula100% (1)