You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Essential Notes in Pain MedicineDocument737 pagesEssential Notes in Pain MedicineRichard Pertwee100% (4)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Synonyms For Words Commonly UsedDocument5 pagesSynonyms For Words Commonly UsedEricDenby100% (19)
- International Financial Questionnaire (IFQ) FormDocument4 pagesInternational Financial Questionnaire (IFQ) FormHenrypat Uche Ogbudu100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Burn Patient Management - Clinical Practice GuidelinesDocument47 pagesBurn Patient Management - Clinical Practice GuidelinesAna PNo ratings yet
- Chemistry of Opioids JakiDocument3 pagesChemistry of Opioids Jakidrugdrug0% (1)
- PLAB Obs Gyne MCQsDocument33 pagesPLAB Obs Gyne MCQsHenrypat Uche Ogbudu100% (3)
- ICNP 2017-Catalogue Disaster NursingDocument27 pagesICNP 2017-Catalogue Disaster NursingHaniv Prasetya Adhi100% (1)
- Pain Management: Kim L. Paxton MSN, ANP, APRN-BC Bro. Jim O'Brien, OFM, Conv. R.N., M.S.N., O.C.NDocument69 pagesPain Management: Kim L. Paxton MSN, ANP, APRN-BC Bro. Jim O'Brien, OFM, Conv. R.N., M.S.N., O.C.NsmusquizNo ratings yet
- E Liberate 2Document329 pagesE Liberate 2noor qureshiNo ratings yet
- Pain Management - 03-07 VersionDocument51 pagesPain Management - 03-07 VersionanreilegardeNo ratings yet
- Recalls 1 Exam Nursing Practice 1: Name: Date: SCOREDocument7 pagesRecalls 1 Exam Nursing Practice 1: Name: Date: SCOREWILMAR DEL MONTE50% (2)
- RMO Skills ListDocument1 pageRMO Skills ListHenrypat Uche OgbuduNo ratings yet
- 2013AminoglycosideDosingGuide PDFDocument2 pages2013AminoglycosideDosingGuide PDFFelipe SotoNo ratings yet
- FormDocument7 pagesFormHenrypat Uche OgbuduNo ratings yet
- RMO Skills ListDocument2 pagesRMO Skills ListHenrypat Uche OgbuduNo ratings yet
- What To Do After PlabDocument2 pagesWhat To Do After PlabnaeamzNo ratings yet
- Introducing Dung Beetles to PasturesDocument3 pagesIntroducing Dung Beetles to PasturesdarylNo ratings yet
- Treatment of Neuropathic Pain MMIGDocument1 pageTreatment of Neuropathic Pain MMIGHenrypat Uche OgbuduNo ratings yet
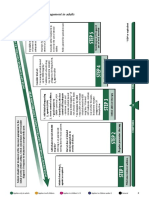
- Summary of Stepwise Management in AdultsDocument3 pagesSummary of Stepwise Management in AdultsHenrypat Uche OgbuduNo ratings yet
- Requirements VisaDocument2 pagesRequirements VisaHenrypat Uche OgbuduNo ratings yet
- Statement U PurposeDocument2 pagesStatement U PurposeHenrypat Uche Ogbudu100% (1)
- Statemenu Purpose PDFDocument2 pagesStatemenu Purpose PDFHenrypat Uche OgbuduNo ratings yet
- PLAB Topics To Be CoveredDocument8 pagesPLAB Topics To Be CoveredHenrypat Uche OgbuduNo ratings yet
- GMC Specimen Questions For PLABDocument8 pagesGMC Specimen Questions For PLABHenrypat Uche OgbuduNo ratings yet
- Psychiatry Imp Topics & NotesDocument4 pagesPsychiatry Imp Topics & NotesHenrypat Uche OgbuduNo ratings yet
- July 2004 Sbas Plab Emqs SbaDocument12 pagesJuly 2004 Sbas Plab Emqs SbaDrZahir UmarNo ratings yet
- Print TotalDocument1 pagePrint TotalHenrypat Uche OgbuduNo ratings yet
- INTERNAL MEDICINE Imp Topics PDFDocument6 pagesINTERNAL MEDICINE Imp Topics PDFHenrypat Uche OgbuduNo ratings yet
- AbstractDocument1 pageAbstractHenrypat Uche OgbuduNo ratings yet
- AndreDocument8 pagesAndreHenrypat Uche OgbuduNo ratings yet
- Application Letter - ST NicholasDocument1 pageApplication Letter - ST NicholasHenrypat Uche OgbuduNo ratings yet
- Professional TrainingDocument1 pageProfessional TrainingHenrypat Uche OgbuduNo ratings yet
- Abia State UniversityDocument1 pageAbia State UniversityHenrypat Uche OgbuduNo ratings yet
- Last TypedDocument2 pagesLast TypedHenrypat Uche OgbuduNo ratings yet
- PC Keyboard Shortcuts PDFDocument1 pagePC Keyboard Shortcuts PDFSelvaraj VillyNo ratings yet
- Professional TrainingDocument1 pageProfessional TrainingHenrypat Uche OgbuduNo ratings yet
- Scope of HRM: 1. The Labour or Personnel AspectDocument4 pagesScope of HRM: 1. The Labour or Personnel AspectHenrypat Uche OgbuduNo ratings yet
- NDDC Foreign Scholarship ProgramDocument2 pagesNDDC Foreign Scholarship ProgramHenrypat Uche Ogbudu100% (1)
- Emphasis On Non-Pharmacologic Aspect: Key Principles: o Gate Control & Neuromatrix Theory of PainDocument3 pagesEmphasis On Non-Pharmacologic Aspect: Key Principles: o Gate Control & Neuromatrix Theory of PainJudy Ignacio EclarinoNo ratings yet
- Assessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective Short TermDocument1 pageAssessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective Short TermTrishia Mae GallardoNo ratings yet
- Mount Hope Ministry of Health Inspection ReportDocument55 pagesMount Hope Ministry of Health Inspection ReportmatthewtrevithickNo ratings yet
- Music Therapy in Acute and Chronic Pain Management: A Literature ReviewDocument2 pagesMusic Therapy in Acute and Chronic Pain Management: A Literature ReviewSean EurekaNo ratings yet
- Minimally Invasive Spine InterventionsDocument8 pagesMinimally Invasive Spine Interventionssanjay chhawraNo ratings yet
- State of Utah v. Purdue Pharma ComplaintDocument54 pagesState of Utah v. Purdue Pharma ComplaintKUER NewsNo ratings yet
- Ajon Music Therapy PresentationDocument10 pagesAjon Music Therapy Presentationapi-383804230No ratings yet
- Adults Exam 1 Practice QuestionsDocument9 pagesAdults Exam 1 Practice QuestionsShenNo ratings yet
- Critical Review On Pentazocine AbuseDocument10 pagesCritical Review On Pentazocine Abuseאדיטי פאווארNo ratings yet
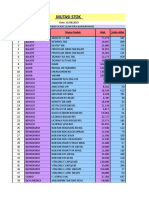
- Mutasi Stok PT Sumber Sehat SejahteraDocument13 pagesMutasi Stok PT Sumber Sehat Sejahteraskapula okNo ratings yet
- NCP Acute Pain Rhea FinalDocument1 pageNCP Acute Pain Rhea FinalSolsona Natl HS MaanantengNo ratings yet
- Fracturas TraumaDocument8 pagesFracturas Traumajoseaugustorojas9414No ratings yet
- What Is Photomedicine?: Important FactsDocument6 pagesWhat Is Photomedicine?: Important FactsidaNo ratings yet
- Analysis Epidural Analgesia Intra Operative Cocktail Pain Management Knee Replacement TKRDocument7 pagesAnalysis Epidural Analgesia Intra Operative Cocktail Pain Management Knee Replacement TKRSSR-IIJLS JournalNo ratings yet
- OxfordMedicineLIVETitleList Aug 2018Document297 pagesOxfordMedicineLIVETitleList Aug 2018Anonymous BOXUxa0% (1)
- The Virtual Meditative Walk: Virtual Reality Therapy For Chronic Pain ManagementDocument5 pagesThe Virtual Meditative Walk: Virtual Reality Therapy For Chronic Pain ManagementMiquel Porcel BareaNo ratings yet
- Dolphin Neurostim Brochure Professional Web PDFDocument2 pagesDolphin Neurostim Brochure Professional Web PDFNeptune ShellNo ratings yet
- Opioid Use Disorder: A VA Clinician's Guide To Identification and Management of Opioid Use Disorder (2016)Document20 pagesOpioid Use Disorder: A VA Clinician's Guide To Identification and Management of Opioid Use Disorder (2016)Hollman Salamanca DimasNo ratings yet
- Thesis Topics in Pain ManagementDocument6 pagesThesis Topics in Pain Managementanamorganfortworth100% (1)
- CV NyeriDocument1 pageCV NyeriMuhammad YunusNo ratings yet
- Opioids, Pain, and FearDocument3 pagesOpioids, Pain, and FearlucianaclarkNo ratings yet
- 37420046-Ncp-Head-Injury 2Document3 pages37420046-Ncp-Head-Injury 2Giselle Chloe Baluya icoNo ratings yet