You might also like
- Allied EPV100 Operation and MaDocument33 pagesAllied EPV100 Operation and Maبشير المتوكلNo ratings yet
- Anesthesia MachineDocument13 pagesAnesthesia MachineCr médicaNo ratings yet
- 21 Neptune PlusDocument4 pages21 Neptune PlusAbhinav DuttaNo ratings yet
- B 5Document8 pagesB 5Edson Lima CharlesNo ratings yet
- Newport e 360 VentilatorDocument6 pagesNewport e 360 VentilatorNeil AcostaNo ratings yet
- Advanced RSSDocument5 pagesAdvanced RSSTECNIMED SYSTEMNo ratings yet
- Superstar S1100: ICU VentilatorDocument8 pagesSuperstar S1100: ICU VentilatorRay FNNo ratings yet
- NL Back Pressure Valve Brochure 032613Document9 pagesNL Back Pressure Valve Brochure 032613EquilibarNo ratings yet
- EPV 200 VentilatorDocument37 pagesEPV 200 VentilatorYash ChoudharyNo ratings yet
- Unit 4Document77 pagesUnit 420BM002 AKSHAYANo ratings yet
- NLB Back Pressure Valves Brochure 032613Document9 pagesNLB Back Pressure Valves Brochure 032613EquilibarNo ratings yet
- 740 Ventilator SystemDocument8 pages740 Ventilator SystemJose Ivan Carvajal CortizosNo ratings yet
- Brosure FalconSEDocument12 pagesBrosure FalconSEBambang ApryantoNo ratings yet
- Pressure Independent Control ValveDocument16 pagesPressure Independent Control ValverakamechNo ratings yet
- Oxymag EnglishDocument40 pagesOxymag EnglishAlauddin SyahNo ratings yet
- Types of Mechanical Ventilators PDFDocument16 pagesTypes of Mechanical Ventilators PDFAnonymous huHDIZyNo ratings yet
- VentilatorDocument9 pagesVentilatorSheeba StephenNo ratings yet
- Ventiladores - Puritan Bennett 760 - BrochureDocument6 pagesVentiladores - Puritan Bennett 760 - BrochureCarlos Mesa Mesa75% (4)
- 403-1 VersamedLM IventDocument9 pages403-1 VersamedLM IventCARLOS2285No ratings yet
- Manual Newport Breeze E150 9493Document63 pagesManual Newport Breeze E150 9493minhhoan200660% (5)
- Lab Report: University of Enginering and Techonology, LahoreDocument20 pagesLab Report: University of Enginering and Techonology, LahoremjunaidNo ratings yet
- IMPACTDocument20 pagesIMPACTmochkurniawanNo ratings yet
- Department of Pediatrics: Specifications of Nasal Cpap MachineDocument4 pagesDepartment of Pediatrics: Specifications of Nasal Cpap MachinenaveenNo ratings yet
- Avance: Clarity of View. - .Clarity of DecisionDocument15 pagesAvance: Clarity of View. - .Clarity of DecisionDevi SadrakhNo ratings yet
- Simple Easy Manufacturable Ventilator Design: Data Collection UnitDocument4 pagesSimple Easy Manufacturable Ventilator Design: Data Collection UnitMuneeb Ur RehmanNo ratings yet
- Allied Mcv100 ManualDocument36 pagesAllied Mcv100 ManualRigneshvaren ThangamoneyNo ratings yet
- CCV-PA500 Ventilator: User'S ManualDocument24 pagesCCV-PA500 Ventilator: User'S ManualDewangga DiraNo ratings yet
- Siaretron 4000 Icu: Intensive Care VentilatorDocument8 pagesSiaretron 4000 Icu: Intensive Care VentilatorHaithamNo ratings yet
- Ventilation Therapy Without CompromiseDocument6 pagesVentilation Therapy Without CompromiseFernandoAdriánNo ratings yet
- Nursing Care of Clients On Mechanical Ventilator For BSN IV StudentsDocument52 pagesNursing Care of Clients On Mechanical Ventilator For BSN IV Studentsspanishthingz01No ratings yet
- Savina BroucherDocument6 pagesSavina Broucheree113051No ratings yet
- In-Situ Fermentors CatalogueDocument4 pagesIn-Situ Fermentors CatalogueVineet GuptaNo ratings yet
- Extremely High Operation Speed European-And US-PatentDocument5 pagesExtremely High Operation Speed European-And US-PatentPeter TvardzíkNo ratings yet
- PA500 Medical Ventilator: Superior Ventilation From ExperienceDocument11 pagesPA500 Medical Ventilator: Superior Ventilation From ExperienceYesy NurNo ratings yet
- PA500 Medical Ventilator: Superior Ventilation From ExperienceDocument11 pagesPA500 Medical Ventilator: Superior Ventilation From ExperienceMita NisaNo ratings yet
- Dragonfly CatalogueDocument4 pagesDragonfly CatalogueABHINANDAN SHARMANo ratings yet
- Volume Booster, Qev and Fail Safe OperationDocument16 pagesVolume Booster, Qev and Fail Safe OperationharishcsharmaNo ratings yet
- Outline Overview of SERVOi EN USDocument12 pagesOutline Overview of SERVOi EN USDimi DimoNo ratings yet
- Servo S Product Brochure en Non Us en Non UsDocument12 pagesServo S Product Brochure en Non Us en Non UsஅNo ratings yet
- User ManualDocument26 pagesUser ManualRodney CutinhoNo ratings yet
- V60 For Invasive VentilationDocument13 pagesV60 For Invasive Ventilationsam samiNo ratings yet
- In-Press: Industrial Style Digital Pressure Meters and ControllersDocument4 pagesIn-Press: Industrial Style Digital Pressure Meters and ControllersMauricio GuanellaNo ratings yet
- 20 Mechanical VentillatorDocument12 pages20 Mechanical VentillatorHamzah AlbrakaniNo ratings yet
- 20 OT-1 Anesthesia Machine With Ventilator& MonitorDocument12 pages20 OT-1 Anesthesia Machine With Ventilator& MonitorHamzah AlbrakaniNo ratings yet
- Ventilador MAXTECDocument19 pagesVentilador MAXTECsantiago rpo cNo ratings yet
- Ventilator Equipment: Industry: Medical Application: VentilatorDocument2 pagesVentilator Equipment: Industry: Medical Application: VentilatorArtem 521No ratings yet
- Basic Principles of MVDocument19 pagesBasic Principles of MVlady birdNo ratings yet
- Festo VPPM Fast Switching SolenoidsDocument58 pagesFesto VPPM Fast Switching Solenoidst8e7w2koNo ratings yet
- Equipment Catalogue 2019 ENDocument24 pagesEquipment Catalogue 2019 ENsangcheolNo ratings yet
- Anesthesia Machine HassamDocument3 pagesAnesthesia Machine HassamHassam ZulfiqarNo ratings yet
- WebPage PDFDocument6 pagesWebPage PDFCláudio Fernando OliveiraNo ratings yet
- Picospritzer ManualDocument17 pagesPicospritzer ManualLívea GodoyNo ratings yet
- Broschuere GB APUS 2020 10Document12 pagesBroschuere GB APUS 2020 10Farahat KhanNo ratings yet
- 3e Ventilator PDFDocument6 pages3e Ventilator PDFNgoc Hau Pham ThiNo ratings yet
- Ventilator PintaDocument43 pagesVentilator PintaDikka AzizNo ratings yet
- Mechanical Ventilation 16-3Document40 pagesMechanical Ventilation 16-3Ahmed Shawky Mohammedin100% (1)
- Arrow ACAT™ 2 Wave® Intra Aortic Balloon Pump: SpecificationsDocument4 pagesArrow ACAT™ 2 Wave® Intra Aortic Balloon Pump: SpecificationsJefford Klein GogoNo ratings yet
- PNEUMATICS AND AIR CIRCUITS UNDERSTANDING THE CASCADE VALVE AND PLC UNDERSTANDINGFrom EverandPNEUMATICS AND AIR CIRCUITS UNDERSTANDING THE CASCADE VALVE AND PLC UNDERSTANDINGNo ratings yet
- Contemporary Anaesthetic Equipments.: An Aid for Healthcare ProfessionalsFrom EverandContemporary Anaesthetic Equipments.: An Aid for Healthcare ProfessionalsNo ratings yet
- Prevention of Actuator Emissions in the Oil and Gas IndustryFrom EverandPrevention of Actuator Emissions in the Oil and Gas IndustryNo ratings yet
- Six Sigma IntroDocument4 pagesSix Sigma Introsingh.abhi08No ratings yet
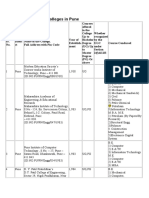
- Engineering Colleges in PuneDocument8 pagesEngineering Colleges in Punepatel_vicky87No ratings yet
- Wind Energy Systems (Johnson)Document449 pagesWind Energy Systems (Johnson)Mario Shawn Hayden Jr100% (1)
- "Connecting The Next Billion People" by ExtendingDocument29 pages"Connecting The Next Billion People" by Extendingpatel_vicky87No ratings yet
- A Hacker's Guide To The InternetDocument14 pagesA Hacker's Guide To The Internetpatel_vicky87No ratings yet
- Surface ModelingDocument6 pagesSurface Modelingpatel_vicky87No ratings yet
- This Leaflet Is For People Who Cut Up or RepairDocument12 pagesThis Leaflet Is For People Who Cut Up or Repairpatel_vicky87No ratings yet
- Transfer Function (Control Engg)Document18 pagesTransfer Function (Control Engg)patel_vicky87100% (1)
- NC Programming VikDocument36 pagesNC Programming Vikpatel_vicky87No ratings yet
- Using Tutorials Tutorial 1in MM Tutorial 1in Inch Tutorial 2Document55 pagesUsing Tutorials Tutorial 1in MM Tutorial 1in Inch Tutorial 2patel_vicky87100% (1)
- Block Diagrams EnotesDocument7 pagesBlock Diagrams Enotespatel_vicky87No ratings yet
- (Ebook) Making and Testing Biodiesel Made Using EthanolDocument23 pages(Ebook) Making and Testing Biodiesel Made Using EthanolkaamaraajanNo ratings yet
- NC Programming VikDocument36 pagesNC Programming Vikpatel_vicky87No ratings yet
- Using Tutorials Tutorial 1in MM Tutorial 1in Inch Tutorial 2Document60 pagesUsing Tutorials Tutorial 1in MM Tutorial 1in Inch Tutorial 2patel_vicky87No ratings yet
- Forensic ScienceDocument16 pagesForensic Sciencepatel_vicky87100% (1)
- STEER Weaning Protocol 3-2002Document45 pagesSTEER Weaning Protocol 3-2002patel_vicky87No ratings yet
- Safety in Gas Cutting & WeldingDocument16 pagesSafety in Gas Cutting & WeldingMitesh MarvaniyaNo ratings yet
- Morris Vent SynchDocument38 pagesMorris Vent Synchpatel_vicky87No ratings yet
- Brief Overview of BTeV Pixel Detector SystemDocument11 pagesBrief Overview of BTeV Pixel Detector Systempatel_vicky87No ratings yet
- Peter Standish SP SolutionsDocument28 pagesPeter Standish SP Solutionspatel_vicky87No ratings yet
- Pumps Ions ModifiedDocument20 pagesPumps Ions Modifiedpatel_vicky87No ratings yet
- AirconditionerDocument2 pagesAirconditionerpatel_vicky87No ratings yet
- Dinesh MohanDocument18 pagesDinesh Mohanpatel_vicky87No ratings yet
- Review Vacuum FinalDocument17 pagesReview Vacuum Finalpatel_vicky87No ratings yet
- 1.design of Camless EngineDocument94 pages1.design of Camless EngineMehul JoganiNo ratings yet
- Pratik Seminar Final 2003Document19 pagesPratik Seminar Final 2003patel_vicky87No ratings yet
- Project Seminar Phase 2Document39 pagesProject Seminar Phase 2patel_vicky87No ratings yet
- As A Man Thinketh - James AllenDocument28 pagesAs A Man Thinketh - James Allenpatel_vicky87No ratings yet
- Crashing Testing of CarsDocument23 pagesCrashing Testing of Carspatel_vicky87No ratings yet
- Tide Power Products50HzDocument22 pagesTide Power Products50HzmaherNo ratings yet
- Iraudamp 16Document26 pagesIraudamp 16Carlos AlvarezNo ratings yet
- Read This FirstDocument21 pagesRead This FirstNíkolas BorgesNo ratings yet
- An Intelligent Algorithm For The Protection of Smart Power SystemsDocument8 pagesAn Intelligent Algorithm For The Protection of Smart Power SystemsAhmed WestministerNo ratings yet
- CLO 1 Scope and Role of SCM in An OrganizationDocument28 pagesCLO 1 Scope and Role of SCM in An OrganizationMelvinNo ratings yet
- How CRM Is The Secret Behind Amazon's SuccessDocument5 pagesHow CRM Is The Secret Behind Amazon's SuccessEduard Magurianu100% (2)
- Forage Compactor 7700: Part of The FC7000 Series of Hay PressesDocument4 pagesForage Compactor 7700: Part of The FC7000 Series of Hay PressesAbimelec TaipeNo ratings yet
- Upload 01767899 1508328417980Document30 pagesUpload 01767899 1508328417980Amine BiomédicalNo ratings yet
- Aeg DC 2000 enDocument2 pagesAeg DC 2000 enmauriceauNo ratings yet
- Miss Komal Ranvir: ObjectiveDocument1 pageMiss Komal Ranvir: ObjectiveKomal RanvirNo ratings yet
- DynaLift 3 6 User Guide A4Document53 pagesDynaLift 3 6 User Guide A4Quy HoangNo ratings yet
- FMEADocument3 pagesFMEAyadiNo ratings yet
- Software Engineering: UNIT-3Document41 pagesSoftware Engineering: UNIT-3Jayavarapu Karthik JNo ratings yet
- Aruba AP-300 Series and AP-207: Ellie Huang, Sr. Product Marketing ManagerDocument11 pagesAruba AP-300 Series and AP-207: Ellie Huang, Sr. Product Marketing Managerarelyta8123No ratings yet
- BHMN SVI3 IOM 34587C 0421 EnglishDocument123 pagesBHMN SVI3 IOM 34587C 0421 Englishgasser ahmedNo ratings yet
- PS2103 Electrical Transients in Power SystemsDocument4 pagesPS2103 Electrical Transients in Power Systemssathishkumar3ramasamNo ratings yet
- YAMAHA P121 SmartPianist - Specification - For202101Document2 pagesYAMAHA P121 SmartPianist - Specification - For202101Romélio LustozaNo ratings yet
- Cable Tray SystemsDocument7 pagesCable Tray SystemsRane SiddeshNo ratings yet
- Roy T. Fielding ThesisDocument7 pagesRoy T. Fielding Thesisjessicahillnewyork100% (2)
- Student User Manual v8 1 PDFDocument23 pagesStudent User Manual v8 1 PDFdaliaNo ratings yet
- Internship Report at A Telecommunication Company / SyriaDocument5 pagesInternship Report at A Telecommunication Company / Syriawaelmahainy10% (1)
- GPON OLT (P1201 08 1.0) User Manual Quick Configuration GuideDocument34 pagesGPON OLT (P1201 08 1.0) User Manual Quick Configuration GuideFedePonceDaminatoNo ratings yet
- SMPBPO102 - 005 v2014 QCCIDocument22 pagesSMPBPO102 - 005 v2014 QCCIJanine Sabio CardonaNo ratings yet
- Datasheet of DS-KIS204 Video Door Phone V1.1.0 20180502 PDFDocument3 pagesDatasheet of DS-KIS204 Video Door Phone V1.1.0 20180502 PDFNareshNo ratings yet
- Petrel 2013 Installation GuideDocument86 pagesPetrel 2013 Installation GuideFebriana Fiona RizkyNo ratings yet
- It Era Final ModuleDocument103 pagesIt Era Final ModuleLeonso Visto JrNo ratings yet
- Interdomain Multicast Soln Guide 1587050838Document336 pagesInterdomain Multicast Soln Guide 1587050838Balaji RajagopalNo ratings yet
- Radio Resource ManagementDocument37 pagesRadio Resource ManagementWahyu KurniawanNo ratings yet
- Electrical Inspection Checklist ConstructionDocument2 pagesElectrical Inspection Checklist ConstructionAtul NikaljeNo ratings yet
- Visvesvaraya Technological University Belagavi - 590018: Developments in Solar Dryers, Collectors and Absorber MaterialsDocument1 pageVisvesvaraya Technological University Belagavi - 590018: Developments in Solar Dryers, Collectors and Absorber MaterialsM.A rajaNo ratings yet