You might also like
- Senam LafiskaDocument6 pagesSenam LafiskaAyuNo ratings yet
- Case Report: Presenter: Irfan Tri Budi WardhanaDocument64 pagesCase Report: Presenter: Irfan Tri Budi Wardhanaabdul100% (1)
- ENG - Hiperplasia EndometriumDocument19 pagesENG - Hiperplasia EndometriumIrwin FitriansyahNo ratings yet
- Emailing Patologi Anatomi GANGGUAN HEMODINAMIK Trombosis DAN SHOCK - Output PDFDocument38 pagesEmailing Patologi Anatomi GANGGUAN HEMODINAMIK Trombosis DAN SHOCK - Output PDFHaykal FathirrahmanNo ratings yet
- 2010 Integrated - Updated Circulation ACLS Prehospital Fibrinolytic Checklist PDFDocument1 page2010 Integrated - Updated Circulation ACLS Prehospital Fibrinolytic Checklist PDFms_lezahNo ratings yet
- Jurnal Acute Decompensated Heart FailureDocument4 pagesJurnal Acute Decompensated Heart FailureMayang Sri WulandNo ratings yet
- Resume Ect MellyDocument15 pagesResume Ect MellyBunda AlvaroNo ratings yet
- Sdki Slki Siki Risiko Infeksi Diagnosa Intervensi Luaran Risiko InfeksiDocument2 pagesSdki Slki Siki Risiko Infeksi Diagnosa Intervensi Luaran Risiko InfeksiSiti RahmawatiNo ratings yet
- 0 Arrhythmia Arwin PDFDocument53 pages0 Arrhythmia Arwin PDFEvans HansenNo ratings yet
- Bu SuryaniDocument68 pagesBu SuryaniMaulana SaputraNo ratings yet
- AKI & Indikasi CRRTDocument25 pagesAKI & Indikasi CRRTMaya Sari BaharumNo ratings yet
- Askep MCI - AchirmanDocument53 pagesAskep MCI - AchirmanmarthaNo ratings yet
- Asuhan Keperawatan Acute Respiratory Distress Syndrome (ARDS)Document20 pagesAsuhan Keperawatan Acute Respiratory Distress Syndrome (ARDS)Hendra Kurnia Rakhma100% (1)
- Manuscript Head Up 30Document9 pagesManuscript Head Up 30Rahmat BudianaNo ratings yet
- Keseimbangan Asam Basa CMDocument47 pagesKeseimbangan Asam Basa CMsyakurNo ratings yet
- Diagnosis Dan Tatalaksana Syok Di Layanan Primer: Rs Pratama Teluk KeramatDocument45 pagesDiagnosis Dan Tatalaksana Syok Di Layanan Primer: Rs Pratama Teluk KeramatNight BaronNo ratings yet
- Monitor Hemodinamik: Pembicara: Dr. Humisar SP - AnDocument95 pagesMonitor Hemodinamik: Pembicara: Dr. Humisar SP - AnaaNo ratings yet
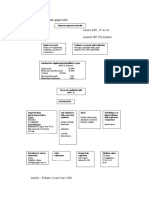
- Algoritma Penatalaksanaan Gagal NafasDocument2 pagesAlgoritma Penatalaksanaan Gagal NafasLion Sangkut Neng EndiNo ratings yet
- Anatomi Sistem KardiovaskularDocument71 pagesAnatomi Sistem KardiovaskularGunk Iztrie Julia TensadianiNo ratings yet
- REVISI 1st Announcement Book 27th ASMIHA 2018 - 12des2017Document21 pagesREVISI 1st Announcement Book 27th ASMIHA 2018 - 12des2017Jimmy Oi SantosoNo ratings yet
- Evita XL ModesDocument2 pagesEvita XL ModesJohn JohnsonNo ratings yet
- Edema ParuDocument42 pagesEdema ParuGP RS EMCNo ratings yet
- Role Play DRKDocument6 pagesRole Play DRKJannatu RNo ratings yet
- Anatomi Fisiologi Pernapasan Dr. MDocument87 pagesAnatomi Fisiologi Pernapasan Dr. MARIF BSNo ratings yet
- Venous Air Embolism (Vae)Document11 pagesVenous Air Embolism (Vae)Andini RizkyNo ratings yet
- Interaksi Jantung ParuDocument29 pagesInteraksi Jantung ParuSusilo Aja100% (1)
- Terapi OksigenDocument12 pagesTerapi OksigenYohana SepthiyaNo ratings yet
- Indikasi Dan Kontraindikasi Dekompresi JarumDocument3 pagesIndikasi Dan Kontraindikasi Dekompresi JarumNurul AtiqahNo ratings yet
- Syok NeurogenikDocument14 pagesSyok NeurogenikFerrany ThiflaNo ratings yet
- Central Line PlacementDocument49 pagesCentral Line PlacementAndresPimentelAlvarezNo ratings yet
- Anatomi Dan Fisiologi TidurDocument25 pagesAnatomi Dan Fisiologi TidurMuhammad HidayatNo ratings yet
- Osteonecrosis Caput FemurDocument23 pagesOsteonecrosis Caput FemurdrhendyjuniorNo ratings yet
- Hubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutDocument7 pagesHubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutnidaNo ratings yet
- LumbotomyDocument25 pagesLumbotomyB2PNo ratings yet
- Patofisiologi Tumor KolonDocument2 pagesPatofisiologi Tumor Kolonnur hijriahNo ratings yet
- Manajemen Shock by FithriDocument59 pagesManajemen Shock by FithriAnonymous YcdK9FWtHNo ratings yet
- Askep in EnglishDocument9 pagesAskep in EnglishnoviNo ratings yet
- Anatomi LimfadenopatiDocument4 pagesAnatomi LimfadenopatioktarinanurfazrianianjasNo ratings yet
- Askep Sirosis HatiDocument48 pagesAskep Sirosis HatiWidya AryantiNo ratings yet
- Acute/Adulth Respiratory Distress Syndrome (ARDS) : RohmanDocument54 pagesAcute/Adulth Respiratory Distress Syndrome (ARDS) : RohmanMuhammad Rizki Junaidi SaputraNo ratings yet
- Stress Ulcer Ditinjau Dari Aspek Patofisiologi Dan TreatmentDocument16 pagesStress Ulcer Ditinjau Dari Aspek Patofisiologi Dan TreatmentJufri NstNo ratings yet
- Management of ACS Complicated With Acute Heart Failure DR BudianaDocument27 pagesManagement of ACS Complicated With Acute Heart Failure DR BudianaLuh Leni AriniNo ratings yet
- SSTi Diabetic PETRI 2019Document36 pagesSSTi Diabetic PETRI 2019intermoska soloNo ratings yet
- Pathway HemoroidDocument1 pagePathway HemoroidAnnisNo ratings yet
- Congestive Heart Failure !1 Running Head: Congestive Heart FailureDocument11 pagesCongestive Heart Failure !1 Running Head: Congestive Heart Failureapi-543558169No ratings yet
- Pemeriksaan Fisik VaskulerDocument25 pagesPemeriksaan Fisik VaskulerTiodora Wike Ds100% (3)
- Terapi Cairan Pada Pasien Shock HemooragikDocument41 pagesTerapi Cairan Pada Pasien Shock HemooragikNur Syifa FadhilahNo ratings yet
- Postmortem Biochemistry of Vitreous Humor and Glucose MetabolismDocument7 pagesPostmortem Biochemistry of Vitreous Humor and Glucose MetabolismsbeyeforhireNo ratings yet
- MINDMAP KEPERAWATAN MEDIKAL BEDAH - CompressedDocument42 pagesMINDMAP KEPERAWATAN MEDIKAL BEDAH - Compressedsiska asialiNo ratings yet
- Syok NeurogenikDocument12 pagesSyok NeurogenikFreddy PanjaitanNo ratings yet
- Vascular Acces in Hemodyalisi - DR DjoniDocument50 pagesVascular Acces in Hemodyalisi - DR DjoniMohamad ZulfikarNo ratings yet
- 2018 Farmakoterapi Obat-Obatan Emergency v2Document90 pages2018 Farmakoterapi Obat-Obatan Emergency v2saifudinNo ratings yet
- B. InggrisDocument14 pagesB. InggrisVia Eliadora TogatoropNo ratings yet
- Prosedur WSD (Water Seal Drainage)Document44 pagesProsedur WSD (Water Seal Drainage)White GooseNo ratings yet
- Anatomi Dan Fisiologi GinjalDocument33 pagesAnatomi Dan Fisiologi GinjalRizha Zhetira100% (1)
- Death Case II DizaDocument29 pagesDeath Case II DizaJayarasti KusumanegaraNo ratings yet
- Pulmonary EdemaDocument1 pagePulmonary EdemaLeonardo ArboledaNo ratings yet
- Daftar Nutrisi ParenteralDocument6 pagesDaftar Nutrisi Parenteralcitrahdyn100% (1)
- Pathway Snake BiteDocument1 pagePathway Snake BiteAlfian Hari GunawanNo ratings yet
- Shock Syndrome: DR Melkamu BDocument62 pagesShock Syndrome: DR Melkamu BAsteway MesfinNo ratings yet
- Trauma Maksilofacial 63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma MaksilofacialDocument7 pagesTrauma Maksilofacial 63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma MaksilofacialChristian SolihinNo ratings yet
- Trauma Maksilofacial 63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma MaksilofacialDocument7 pagesTrauma Maksilofacial 63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma MaksilofacialChristian SolihinNo ratings yet
- Kar Dio VasaDocument6 pagesKar Dio VasaArif NurfadhilahNo ratings yet
- Kardiovasa 2Document8 pagesKardiovasa 2Arif NurfadhilahNo ratings yet
- Peranan Cairan Perioperative RevDocument27 pagesPeranan Cairan Perioperative RevRuswendra PermanaNo ratings yet
- CpeDocument21 pagesCpeArif NurfadhilahNo ratings yet
- CpeDocument21 pagesCpeArif NurfadhilahNo ratings yet
- Maternity3Document7 pagesMaternity3Arif NurfadhilahNo ratings yet
- Maternity3Document7 pagesMaternity3Arif NurfadhilahNo ratings yet
- Evaluation and Management of Suspected Sepsis and Septic Shock in AdultsDocument62 pagesEvaluation and Management of Suspected Sepsis and Septic Shock in AdultsGiussepe Chirinos CalderonNo ratings yet
- Choque y Receptores AdrenergicosDocument9 pagesChoque y Receptores AdrenergicosJoelGámezNo ratings yet
- Treatment of Streptococcal Toxic Shock SyndromeDocument4 pagesTreatment of Streptococcal Toxic Shock SyndromeAlbertoMarteNo ratings yet
- Burn-Like Skin Necrosis in A Patient Following Infusion of Sodium BicarbonateDocument3 pagesBurn-Like Skin Necrosis in A Patient Following Infusion of Sodium BicarbonateViniFortunataNo ratings yet
- Shock - Classification and Pathophysiological Principles of TherapeuticsDocument12 pagesShock - Classification and Pathophysiological Principles of TherapeuticsLuis ChancusigNo ratings yet
- Shock AssessmentDocument36 pagesShock AssessmentAlyssandra LucenoNo ratings yet
- Jurnal Kritis 6 PDFDocument5 pagesJurnal Kritis 6 PDFEndah Novianti SoenarsinNo ratings yet
- Chapter Review: True or FalseDocument2 pagesChapter Review: True or FalseJames Gabriel SalardaNo ratings yet
- Use of Vasopressors and Inotropes - UpToDateDocument18 pagesUse of Vasopressors and Inotropes - UpToDateAlbertoMarteNo ratings yet
- SCHWARTZ Surgical InfectionDocument25 pagesSCHWARTZ Surgical InfectionAlexandra Niken Larasati78% (9)
- Sepsis 2021Document50 pagesSepsis 2021Dhitiwat ChangNo ratings yet
- The Physiology of ShockDocument37 pagesThe Physiology of ShockGauxy AromboNo ratings yet
- Seminars 2019 PDFDocument200 pagesSeminars 2019 PDFpaingmyintNo ratings yet
- Monitoreo Hemodinamico Funcional PinskyDocument23 pagesMonitoreo Hemodinamico Funcional PinskyJuan CarrascoNo ratings yet
- 017 UrologyDocument544 pages017 UrologyNashaat H. Alshawabkeh100% (2)
- Neonatal Sepsis (NNS) : DR Jerome SiyambuDocument37 pagesNeonatal Sepsis (NNS) : DR Jerome SiyambuEmmanuel MukukaNo ratings yet
- Journal Pediatric IndiaDocument5 pagesJournal Pediatric IndiaHhhNo ratings yet
- Inotropic and Vasoactive Drugs in Pediatric ICUDocument6 pagesInotropic and Vasoactive Drugs in Pediatric ICUCandy RevolloNo ratings yet
- Procalcitonin: For Diagnosis and Guidance of Antibiotic TherapyDocument24 pagesProcalcitonin: For Diagnosis and Guidance of Antibiotic TherapyLilik IndrawatiNo ratings yet
- W2D3 DR - Yasa-Bacteremia Dan SepsisDocument54 pagesW2D3 DR - Yasa-Bacteremia Dan SepsisJaka BawaviNo ratings yet
- Cosmo Fowler Sepsis and Adrenal Insufficiency 2023Document10 pagesCosmo Fowler Sepsis and Adrenal Insufficiency 2023Luis Hernán Guerrero LoaizaNo ratings yet
- Sirs & ModsDocument5 pagesSirs & Modsmarlou agananNo ratings yet
- 132 Emergency MedicineDocument14 pages132 Emergency MedicineVania NandaNo ratings yet
- Sepsis SurvivingDocument16 pagesSepsis SurvivingAlberto MHNo ratings yet
- Multiple Organ Dysfunction SyndromeDocument2 pagesMultiple Organ Dysfunction SyndromeMaryjoy Gabriellee De La CruzNo ratings yet
- Albumin Administration in The Acutely Ill: What Is New and Where Next?Document10 pagesAlbumin Administration in The Acutely Ill: What Is New and Where Next?Peter AgabaNo ratings yet
- ECG Changes During Septic Shock PDFDocument10 pagesECG Changes During Septic Shock PDFandikaisnaeniNo ratings yet
- VasoactivosDocument8 pagesVasoactivosrogelio cruzNo ratings yet
- The Evolving Challenge of Infections in CirrhosisDocument14 pagesThe Evolving Challenge of Infections in Cirrhosiscastillocavazos09No ratings yet
- Sample of MRCOG Assessment 2021 - Saeed HasanDocument28 pagesSample of MRCOG Assessment 2021 - Saeed HasanIslam AwniNo ratings yet