You might also like
- Radiod MasterDocument149 pagesRadiod MasterAhmeid Eid0% (1)
- Chest X-RayDocument101 pagesChest X-RayYuke04No ratings yet
- FC Rad Diag (SA) Part I Past Papers - 2019 2nd Semester 3 1 2020Document2 pagesFC Rad Diag (SA) Part I Past Papers - 2019 2nd Semester 3 1 2020Mo CajeeNo ratings yet
- Test Bank For Radiologic Science For Technologists 12th Edition by BushongDocument51 pagesTest Bank For Radiologic Science For Technologists 12th Edition by Bushongmarcuskenyatta275No ratings yet
- VE026 MECHANICAL MANUAL enDocument33 pagesVE026 MECHANICAL MANUAL enJoséNo ratings yet
- MCQ in AC Circuits Part 1 REE Board ExamDocument18 pagesMCQ in AC Circuits Part 1 REE Board ExamRogelio Jr. Dela CruzNo ratings yet
- Basic QA RadiologyDocument55 pagesBasic QA RadiologyWahyu Widhianto100% (10)
- Doppler Ultrasound of The KidneysDocument23 pagesDoppler Ultrasound of The KidneysivoklarinNo ratings yet
- 103manual QAP Radiologi Pindaan Januari 2019Document115 pages103manual QAP Radiologi Pindaan Januari 2019UMGC Sri RampaiNo ratings yet
- Radio BiologyDocument26 pagesRadio BiologyMAN MedanNo ratings yet
- Ultrasound Equipment Quality Assurance - CHAPTER 14Document3 pagesUltrasound Equipment Quality Assurance - CHAPTER 14Pengcab PARI Kota BekasiNo ratings yet
- PathologyDocument53 pagesPathologyEdwin Mccain100% (1)
- CM X-Ray Film Processor PPDocument19 pagesCM X-Ray Film Processor PPamelia kartikaNo ratings yet
- BiopsyDocument19 pagesBiopsyQendrim BerishaNo ratings yet
- Equipment For X - & Gamma Ray RadiographyDocument42 pagesEquipment For X - & Gamma Ray Radiographymangsuresh100% (1)
- Electrical Safety Book PDFDocument36 pagesElectrical Safety Book PDFhoaithuat100% (1)
- 1.0 The Origin of Biopotentials (New)Document62 pages1.0 The Origin of Biopotentials (New)Hanif HussinNo ratings yet
- Test Bank For Merrills Atlas of Radiographic Positioning and Procedures 13th Edition by LongDocument6 pagesTest Bank For Merrills Atlas of Radiographic Positioning and Procedures 13th Edition by Longdominicmaximus44uNo ratings yet
- Lecture 7 Doppler and HaemodynamicsDocument54 pagesLecture 7 Doppler and HaemodynamicsattooNo ratings yet
- Biological Effects of UltrasoundDocument3 pagesBiological Effects of UltrasoundSaravjeet Singh100% (1)
- Physics Lectures For Residents: MRI ArtifactDocument37 pagesPhysics Lectures For Residents: MRI ArtifactLajja Parikh PatelNo ratings yet
- UZVDocument56 pagesUZVGoran MaliNo ratings yet
- Fluoroscopy Equipment DiagramDocument3 pagesFluoroscopy Equipment Diagramapi-338781568No ratings yet
- Principles of Exposure Ch.8Document42 pagesPrinciples of Exposure Ch.8abdulsalam khalaf100% (1)
- MEDICAL ELECTRONICS PROJECTS ABSTRACT-Digital Pulmonary Function Test - SpirometryDocument4 pagesMEDICAL ELECTRONICS PROJECTS ABSTRACT-Digital Pulmonary Function Test - SpirometryR.ASHOKKUMAARNo ratings yet
- Digital Subtraction AngiographyDocument42 pagesDigital Subtraction AngiographyRoshan Chaudhary100% (1)
- Thesis Setup Error PelvicDocument43 pagesThesis Setup Error PelvichandiaviNo ratings yet
- Module 1 Computed Tomography and Principles of OperationsDocument6 pagesModule 1 Computed Tomography and Principles of OperationsWayne De Vergara PalaypayonNo ratings yet
- Resolution in Ultrasound ImagingDocument7 pagesResolution in Ultrasound ImagingVyshnavi EaswaranNo ratings yet
- Mods of UltrasoundDocument22 pagesMods of UltrasoundEnrique Valdez JordanNo ratings yet
- Contrast Media and Adverse Effects - Vijay KumarDocument41 pagesContrast Media and Adverse Effects - Vijay KumarTapshi SohalNo ratings yet
- Grids and Scatter ReductionDocument79 pagesGrids and Scatter ReductionMondiaal Financial ServicesNo ratings yet
- Diclofenac From Administration To Adverse Effect A Mini-ReviewDocument5 pagesDiclofenac From Administration To Adverse Effect A Mini-ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Chapter 26: Density/Image Receptor Exposure: Notebook #7Document8 pagesChapter 26: Density/Image Receptor Exposure: Notebook #7api-338781568No ratings yet
- Final MIT Logbook JamilDocument15 pagesFinal MIT Logbook Jamilammar-nasir3314No ratings yet
- 1969 - Rossmann - Point Spread-Function, Line Spread-Function, and Modulation Transfer Function. Tools For The Study of Imaging Systems PDFDocument16 pages1969 - Rossmann - Point Spread-Function, Line Spread-Function, and Modulation Transfer Function. Tools For The Study of Imaging Systems PDFClaudio BiaginiNo ratings yet
- Diagnostic Reference Level in Lumbar Radiography in Abidjan, Côte D'ivoireDocument5 pagesDiagnostic Reference Level in Lumbar Radiography in Abidjan, Côte D'ivoiretheijesNo ratings yet
- Iodinated Contrast Media GuidelineDocument41 pagesIodinated Contrast Media GuidelineN Aa100% (1)
- (Philip T. English DCR, Christine Moore DCR (Auth.Document188 pages(Philip T. English DCR, Christine Moore DCR (Auth.Åri Budianto100% (1)
- Spiral CT DR - ShravaniDocument82 pagesSpiral CT DR - ShravaniVajja Swati100% (2)
- Vertebral Column Skull Projection MethodDocument8 pagesVertebral Column Skull Projection MethodLaFranz CabotajeNo ratings yet
- Viner 2005 Forensic Radiography in South AfricaDocument24 pagesViner 2005 Forensic Radiography in South Africah8517No ratings yet
- Gamma CameraDocument48 pagesGamma CameraMarcela OviedoNo ratings yet
- ArtifactDocument3 pagesArtifactfeiflyfly100% (1)
- National Radiologic Technology Licensure Examination PerformanceDocument1 pageNational Radiologic Technology Licensure Examination PerformancePRINCESS MIE SAPELINONo ratings yet
- A-Level: Physics (7408/2)Document14 pagesA-Level: Physics (7408/2)sam gomNo ratings yet
- Osteoarthritis: Uyenvy Pham, M.D. Swedish Geriatric Fellow March 22, 2011Document45 pagesOsteoarthritis: Uyenvy Pham, M.D. Swedish Geriatric Fellow March 22, 2011Saya MenangNo ratings yet
- Trauma Radiography Puteri Resort Melaka 2010Document69 pagesTrauma Radiography Puteri Resort Melaka 2010Syuhada AzmiNo ratings yet
- B-Scan Ocular UltrasoundDocument29 pagesB-Scan Ocular UltrasoundJeanna SalimaNo ratings yet
- Assignment On SI UnitsDocument11 pagesAssignment On SI UnitsAeshwrya Panda0% (1)
- Abdomen CTDocument26 pagesAbdomen CTAnto BijuNo ratings yet
- Reference Books For MDCB Exam ReviewDocument2 pagesReference Books For MDCB Exam ReviewMDCB ExamNo ratings yet
- DR - Shamim Rima MBBS, Dmu, FCGP M.Phil Radiology & Imaging BsmmuDocument46 pagesDR - Shamim Rima MBBS, Dmu, FCGP M.Phil Radiology & Imaging Bsmmudr_shamimr100% (1)
- Ultrasound Machine: Unit C18.6 Maintaining Medical Imaging Equipment 18.6.7 Maintain An Ultrasound MachineDocument17 pagesUltrasound Machine: Unit C18.6 Maintaining Medical Imaging Equipment 18.6.7 Maintain An Ultrasound Machineanwar1971No ratings yet
- Contrast MediaDocument6 pagesContrast MediardmdelarosaNo ratings yet
- Neuropath Exam 3 Practice QuestionsDocument20 pagesNeuropath Exam 3 Practice QuestionsKristin SmithNo ratings yet
- Basic of Doppler UltrasoundDocument25 pagesBasic of Doppler Ultrasoundpepsimax85No ratings yet
- 1stprize CR Auditpostercomp C Reid 2015Document1 page1stprize CR Auditpostercomp C Reid 2015webber_denzNo ratings yet
- The Safe Use of Fluoroscopy: Radiation Protection Ala' ThawabtehDocument41 pagesThe Safe Use of Fluoroscopy: Radiation Protection Ala' ThawabtehDiaa AyobNo ratings yet
- Principles and Practice of Pharmacology for AnaesthetistsFrom EverandPrinciples and Practice of Pharmacology for AnaesthetistsRating: 5 out of 5 stars5/5 (1)
- Introduction To The Physical Principles of Ultrasound Imaging and Doppler Peter N Burns PHDDocument26 pagesIntroduction To The Physical Principles of Ultrasound Imaging and Doppler Peter N Burns PHDCatarina Dos ReisNo ratings yet
- Free Applications Support On Every Voluson 730 Ultrasound Machine PurchaseDocument3 pagesFree Applications Support On Every Voluson 730 Ultrasound Machine PurchaseAhmed SabryNo ratings yet
- GE Logiq 5 ProDocument2 pagesGE Logiq 5 ProAhmed SabryNo ratings yet
- GE Logiq 3 Ultrasound Machine: Contact Us For A QuoteDocument2 pagesGE Logiq 3 Ultrasound Machine: Contact Us For A QuoteAhmed SabryNo ratings yet
- Computer InterfacesDocument68 pagesComputer InterfacesAhmed SabryNo ratings yet
- Brivo BrochureDocument12 pagesBrivo BrochureAhmed SabryNo ratings yet
- Service Manual: Color MonitorDocument3 pagesService Manual: Color MonitorAhmed SabryNo ratings yet
- Linear Accelerators Radiotherapy Units, Cobalt: March 2002Document33 pagesLinear Accelerators Radiotherapy Units, Cobalt: March 2002Ahmed Sabry0% (1)
- Vco-151215121140 Import PPTDocument60 pagesVco-151215121140 Import PPTRizwan SPNo ratings yet
- Standard Heavy Duty Limit Switches FD/FP/FL: Options and Ordering CodesDocument9 pagesStandard Heavy Duty Limit Switches FD/FP/FL: Options and Ordering CodesNisar AhmedNo ratings yet
- OCS DC ApolloDocument13 pagesOCS DC ApolloRuben Rumipamba ZambranoNo ratings yet
- Electrical Tech & Specs ADocument78 pagesElectrical Tech & Specs AAbdillah FadhilNo ratings yet
- 20181201113141Document28 pages20181201113141Galuh PrambananNo ratings yet
- RTN 905Document189 pagesRTN 905mabvieira100% (3)
- DHTDocument9 pagesDHTNoman Jabbar100% (2)
- Iot Based Energy MeterDocument6 pagesIot Based Energy MeterZhak M. MuneneNo ratings yet
- Hostile Duty Motors: Cast Iron Frame, Totally Enclosed Fan CooledDocument2 pagesHostile Duty Motors: Cast Iron Frame, Totally Enclosed Fan CooledJulián GonzálezNo ratings yet
- Fan Regulator CircuitDocument2 pagesFan Regulator CircuitNaeemLatifNo ratings yet
- SIGNALLINGDocument11 pagesSIGNALLINGshiva_nivas0% (1)
- 13.4. Spare Part List of Gekamac GKM 420-2GDocument2 pages13.4. Spare Part List of Gekamac GKM 420-2GBa MamadouNo ratings yet
- Spesifikasi Teknis Elevator Gd. Data Center Divti Polri Cikeas BogorDocument2 pagesSpesifikasi Teknis Elevator Gd. Data Center Divti Polri Cikeas BogorTedi SNo ratings yet
- Solar Catalogue New 2024 - CompressedDocument34 pagesSolar Catalogue New 2024 - Compressedyogendrperjapati61No ratings yet
- IMX6SDLCECDocument169 pagesIMX6SDLCECRaim DelgadoNo ratings yet
- Wm-526 Specification SheetDocument5 pagesWm-526 Specification SheetPiero Fabrizzio Mendoza FuenteNo ratings yet
- MUCLecture 2023 3140165Document9 pagesMUCLecture 2023 3140165hus khNo ratings yet
- Acer Spin 3 SP315-51 Pegatron ST5DB Rev1.0Document82 pagesAcer Spin 3 SP315-51 Pegatron ST5DB Rev1.0ffffNo ratings yet
- GRB200 (Decentralized) Brochure - 18005-G2A-0.10Document39 pagesGRB200 (Decentralized) Brochure - 18005-G2A-0.10krishna mohanNo ratings yet
- RelianceDocument21 pagesRelianceSukanta ParidaNo ratings yet
- Chapter 1Document21 pagesChapter 1iris33% (3)
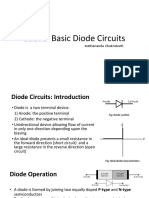
- Diode CircuitsDocument28 pagesDiode CircuitsRatanNo ratings yet
- Servo Gun v2.8 (Eng) ObaraDocument63 pagesServo Gun v2.8 (Eng) Obaralogaing13No ratings yet
- Life Cycle Management of Power Transformers Using Transformer Protection RelayDocument7 pagesLife Cycle Management of Power Transformers Using Transformer Protection RelaycuamiNo ratings yet
- Watchman Oil MonitorDocument6 pagesWatchman Oil MonitorSensors Systems - The Winter Fuel ShopNo ratings yet
- COMAND 2.0, Which Is The CD Based COMAND System Fitted To The W208 CLK, W210 E Class, W220 S Class (Before MY2004)Document4 pagesCOMAND 2.0, Which Is The CD Based COMAND System Fitted To The W208 CLK, W210 E Class, W220 S Class (Before MY2004)AdamNo ratings yet
- Line Protection UnitDocument6 pagesLine Protection Unitsumitverma1990No ratings yet
- Manual TDocument36 pagesManual TAnonymous DiBRT8No ratings yet