You might also like
- Catatan Koas MataDocument54 pagesCatatan Koas MataMuftiNo ratings yet
- Signs That Suggest The Presence or Possibility of OpenDocument3 pagesSigns That Suggest The Presence or Possibility of Openad3_vianis5654No ratings yet
- MR 17 - 10 - 2013 Baru - PpsDocument10 pagesMR 17 - 10 - 2013 Baru - Ppsad3_vianis5654No ratings yet
- A Scribe HGDocument1 pageA Scribe HGad3_vianis5654No ratings yet
- A Scribe HGJJNBBHJHDocument1 pageA Scribe HGJJNBBHJHad3_vianis5654No ratings yet
- LicenseDocument6 pagesLicensemerrysun22No ratings yet
- A Scribe HGDocument1 pageA Scribe HGad3_vianis5654No ratings yet
- A ScribeDocument1 pageA Scribead3_vianis5654No ratings yet
- AapahDocument1 pageAapahad3_vianis5654No ratings yet
- A ScribeDocument1 pageA Scribead3_vianis5654No ratings yet
- A ScribeDocument1 pageA Scribead3_vianis5654No ratings yet
- A ScribeDocument1 pageA Scribead3_vianis5654No ratings yet
- HTTPDocument1 pageHTTPad3_vianis5654No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Onkyo TX NR555 ManualDocument100 pagesOnkyo TX NR555 ManualSudhit SethiNo ratings yet
- Hospitality Marketing Management PDFDocument642 pagesHospitality Marketing Management PDFMuhamad Armawaddin100% (6)
- Monson, Concilio Di TrentoDocument38 pagesMonson, Concilio Di TrentoFrancesca Muller100% (1)
- NewsletterDocument1 pageNewsletterapi-365545958No ratings yet
- Ck-Nac FsDocument2 pagesCk-Nac Fsadamalay wardiwiraNo ratings yet
- Eco Orphanage: Model of Sustainability: 15 536 Words (Not Including Bibliography)Document78 pagesEco Orphanage: Model of Sustainability: 15 536 Words (Not Including Bibliography)Princess ManiquizNo ratings yet
- CVA: Health Education PlanDocument4 pagesCVA: Health Education Plandanluki100% (3)
- Cignal Channel 490Document2 pagesCignal Channel 490Arild JuliusNo ratings yet
- Treatment of Pituitary Adenoma by Traditional Medicine TherapiesDocument3 pagesTreatment of Pituitary Adenoma by Traditional Medicine TherapiesPirasan Traditional Medicine CenterNo ratings yet
- Special Blood CollectionDocument99 pagesSpecial Blood CollectionVenomNo ratings yet
- Booklet - CopyxDocument20 pagesBooklet - CopyxHåkon HallenbergNo ratings yet
- McKesson Point of Use Supply - FINALDocument9 pagesMcKesson Point of Use Supply - FINALAbduRahman MuhammedNo ratings yet
- Unit 5 The Teacher As ProfessionalDocument23 pagesUnit 5 The Teacher As ProfessionalLeame Hoyumpa Mazo100% (5)
- Edpb 506 Intergrated Unit Project RubricDocument1 pageEdpb 506 Intergrated Unit Project Rubricapi-487414247No ratings yet
- Problem Areas in The Inpatient DepartmentDocument2 pagesProblem Areas in The Inpatient DepartmentVineet AgarwalNo ratings yet
- Misbehaviour - Nges Rgyur - I PDFDocument32 pagesMisbehaviour - Nges Rgyur - I PDFozergyalmoNo ratings yet
- MEAB Enewsletter 14 IssueDocument5 pagesMEAB Enewsletter 14 Issuekristine8018No ratings yet
- Math 8 1 - 31Document29 pagesMath 8 1 - 31Emvie Loyd Pagunsan-ItableNo ratings yet
- EDMOTO 4th TopicDocument24 pagesEDMOTO 4th TopicAngel Delos SantosNo ratings yet
- Blood Culture & Sensitivity (2011734)Document11 pagesBlood Culture & Sensitivity (2011734)Najib AimanNo ratings yet
- Asian Paints SmartCare Damp Proof Warranty for TerracesDocument11 pagesAsian Paints SmartCare Damp Proof Warranty for Terracesiman.krisman2109No ratings yet
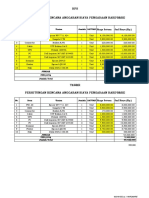
- HPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANDocument2 pagesHPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANYanto AstriNo ratings yet
- Legal Maxim V02Document29 pagesLegal Maxim V02singam harikanthNo ratings yet
- Timpuri Verbale Engleza RezumatDocument5 pagesTimpuri Verbale Engleza RezumatBogdan StefanNo ratings yet
- WEEK 4 A. Family Background of Rizal and Its Influence On The Development of His NationalismDocument6 pagesWEEK 4 A. Family Background of Rizal and Its Influence On The Development of His NationalismVencint LaranNo ratings yet
- Piramal Annual ReportDocument390 pagesPiramal Annual ReportTotmolNo ratings yet
- Identification Guide To The Deep-Sea Cartilaginous Fishes of The Indian OceanDocument80 pagesIdentification Guide To The Deep-Sea Cartilaginous Fishes of The Indian OceancavrisNo ratings yet
- Your Money Personality Unlock The Secret To A Rich and Happy LifeDocument30 pagesYour Money Personality Unlock The Secret To A Rich and Happy LifeLiz Koh100% (1)
- Mitanoor Sultana: Career ObjectiveDocument2 pagesMitanoor Sultana: Career ObjectiveDebasish DasNo ratings yet
- KARTONAN PRODUkDocument30 pagesKARTONAN PRODUkAde SeprialdiNo ratings yet